Order nitroglycerin 6.5 mg with mastercardPositioning and Portals A panlabral restore can be performed in each the beach chair and lateral decubitus place medicine review nitroglycerin 2.5 mg generic with visa. It is paramount to identify and pad all bony prominences and areas of potential nerve compression in the course of the process symptoms tuberculosis cheap nitroglycerin 6.5 mg on line. Specifically, the brachial plexus and the widespread peroneal nerve are susceptible to compression during procedures performed within the lateral decubitus position. An axillary roll must be used to protect the axillary buildings and the lateral knee have to be free of compression all through the process. Prior to sterile preparation and draping, a radical instability exam is carried out once the patient is anesthetized and the airway is protected. Glenohumeral vary of movement, translation, and laxity are assessed relative to the contralateral shoulder. While an examination underneath anesthesia can provide useful data, this examination serves primarily to confirm the preoperative prognosis and surgical plan. The superficial floor anatomy of the shoulder is marked in order to optimize portal placement. The glenohumeral joint is first insufflated with 60 mL of regular saline to find a way to distend the capsule and optimize safe trocar entry. This is especially helpful in these circumstances for the reason that posterior viewing portal is created slightly extra lateral than normal, which facilitates posterior anchor placement on the expense of ease of intra-articular trocar entry. A posterior viewing portal is established approximately 1 cm medial and three cm distal to the posterolateral border of the acromion, with the trocar aimed at the tip of the coracoid. The authors are likely to make this portal slightly more lateral than normal in posterior instability instances as a end result of posterior anchors can usually be placed through this portal. The morbidity of an additional portal is way lower than a poorly accomplished labral repair that was not appropriately executed due to unfavorable portal placement. Once intra-articular placement of the digicam is confirmed, an anterosuperior portal is established with 18-gauge spinal needle localization just anterior to the biceps tendon and just lateral to the coracoid. The arthroscope is switched to the trans-cuff portal and provides a wonderful global view of each the (B) posterior and (C) anterior labrum. A probe is launched and an intensive diagnostic arthroscopy then carried out to quantify the extent of the capsulolabral pathology, establish and quantify glenoid bone loss, and establish any extra intra-articular pathology corresponding to a rotator cuff tear or biceps tendon lesion. An 11-blade scalpel is then used to pierce the superficial skin, deltoid, and supraspinatus according to its fibers, and a blunt switching stick is then launched adopted by an additional 5-mm cannula over the switching stick. The digicam is then switched to the trans-cuff portal, which offers a wonderful world view of the glenoid and labrum, and an 8-mm cannula is changed over a switching stick in the original posterior viewing portal. This portal is usually according to the posterolateral border of the acromion and 2 to 3 cm distal to the unique posterior viewing portal. This portal is purposely more lateral and distal than a traditional posterior portal to find a way to optimize applicable placement of the posterior glenoid anchors. Care should be taken to not injure the axillary nerve throughout portal placement and manipulation. Finally, a mid-glenoid portal is created simply superior to the subscapularis and as lateral as needed to have the ability to optimize anterior glenoid anchor placement. This portal is created after the posterior restore is accomplished since the glenoid and humeral relationship adjustments after the posterior repair/plication is carried out. This is likely crucial side of the restore and ought to be done carefully and fully. A radiofrequency blade device is used to exploit the interval between the labrum and glenoid neck till the rotator cuff muscle is visualized. Care must be taken to maintain the radiofrequency gadget on the glenoid neck and proceed medially on bone. Once the tissues are free, a shaver is used to flippantly debride the glenoid neck free of all soft tissue and right down to bleeding bone. The posterior labrum is addressed first from inferior to superior since this space of the shoulder is normally essentially the most troublesome to entry, and the shoulder turns into progressively tighter because the sutures are tied down. The pores and skin solely is then incised, and the introducer for the anchor is used to pierce the capsule. The amount of capsule captured with the labrum is dependent on the quantity of capsular laxity that the surgeon believes is current, which is often 5 to 10 mm of capsule from the capsulolabral junction. Care have to be taken only to seize capsulolabral tissue with the suture shuttle because the axillary nerve is immediately adjoining to the inferior capsule. The sutures are then retrieved via the posterior portal after which tied after traction is removed from the arm. A sliding, locking knot is utilized with 3 alternating half-hitches, guaranteeing that the knot is as far away from the chondral surface as possible. More aggressive bites of capsule are taken with the inferior suture limb of every of the anchors as opposed to the superior limb to effectively create an inferior capsular shift. A normal Bankart restore is carried out after the capsulolabral tissue is totally mobilized till subscapularis muscle belly is visualized as noted beforehand. The mid-glenoid portal is utilized to place the anchors and move the suture, which is as distal and lateral as attainable simply above the higher border of the subscapularis so as to optimize anchor placement. Similar to the posterior repair, a curved tissue penetrator is used to grasp roughly 5 mm of capsule and labrum. The second suture limb is retrieved through the mid-glenoid portal and then shuttled after the tissue penetrator grasps the anteroinferior glenohumeral ligament in order to create the 1-anchor, 2-simple suture configuration. The sutures are retrieved through the posterior portal so as to keep away from entanglement because the second anchor is handed. The sutures are then sequentially retrieved anteriorly from inferior to superior utilizing a sliding, locking knot with alternating half-hitches maintaining the knot away from the articular floor. The trans-cuff portal provides an optimal angle for superior glenoid anchor placement. A curved tissue penetrator is then used by way of the posterior portal to move 2 easy sutures just posterior to the biceps origin, then tied. A nonabsorbable suture is grasped by a straight tissue penetrator, and the superior interval tissue adjacent to the forefront of the supraspinatus is pierced utilizing the anterosuperior portal roughly 1 cm medial from the biceps pulley. The suture is "parked" within the joint, the penetrator is withdrawn from the tissue, inferior interval tissue is penetrated just above the subscapularis, and the suture is retrieved from the joint. The suture is then tied blindly, however the interval closure is visualized as the suture is cinched down. A complete analysis of the labral repair with a probe is performed to verify anatomic restoration of the labrum and appropriate capsular tension. Postoperative Protocol Regional anesthesia is encouraged for acute postoperative pain control. Patients are routinely positioned in a shoulder immobilizer in external rotation for six weeks so as to defend the labral restore anteriorly and posteriorly. Patients may take away the sling only for hygiene and are instructed on the method to hold the shoulder in external rotation and the elbow fixed on the iliac crest while showering.
Banafshah (Sweet Violet). Nitroglycerin. - How does Sweet Violet work?
- Dosing considerations for Sweet Violet.
- Asthma, bronchitis, colds, congestion, cough, depression, flu symptoms, sleeplessness, lung problems, menopausal symptoms, nervousness, stomach problems, urinary problems, and other conditions.
- Are there safety concerns?
- What is Sweet Violet?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96245
2.5 mg nitroglycerin order amexThe large sensory pathways of the spinal wire (the tracts of the dorsal column) are relayed to the nuclei cuneatus and gracilus medications not to take when pregnant 2.5 mg nitroglycerin buy overnight delivery, which send their axons through the medial lemniscus to terminate within the ventral posterolateral nucleus (4) symptoms 6 year molars nitroglycerin 6.5 mg discount free shipping, while the trigeminal sensory pathways from the head terminate within the ventral posterom edial nucleus (5, trigem inal lemniscus, see p. Topographical localization based on perform is a primary principle of neural group. Anterior thalam ic radiation Central thalam ic radiation Posterior thalam ic radiation Intralam inar nuclei Specific thalam ic nuclei Centrom edian nucleus Reticular nucleus F Nonspeci c thalamic nuclei Coronal sections presented in an oral-to-caudal sequence. The nonspecic thalam ic nuclei project to the brainstem, to other nuclei in the diencephalon (including other thalam ic nuclei), and to the corpus striatum. The m edial nonspecif c thalam ic nuclei are sub divided into t wo groups: � Nuclei of the central thalam ic gray m at ter (m idline nuclei): sm all groups of cells distributed along the wall of the third ventricle � Intralam inar nuclei, positioned within the inner m edullary lam ina. The lateral specif c thalam ic nucleus shown in the diagram is the reticular nucleus of the thalam us, which is located lateral to the opposite speci c thalam ic nuclei. Inferior thalam ic radiation G Thalamic radiations Lateral ventricle of the left hem isphere. The axons of the speci c thalam ic nuclei (so referred to as because their bers project to speci c cortical areas) are collected into tract s that type the thalam ic radiations. The arrangem ent of the bers exhibits that the speci c thalam ic nuclei have connections with all areas of the cortex. The anterior thalam ic radiation projects to the frontal lobe, the central thalam ic radiation to the parietal lobe, the posterior thalam ic radiation to the occipital lobe, and the inferior thalam ic radiation to the temporal lobe. It incorporates sensory bers for position sense, vibration, strain, discrim ination, and touch that are relayed from the nucleus gracilis and nucleus cuneatus. The anterior nucleus establishes both a erent and e erent connections with the cingulate gyrus of the telencephalon. The largest nonspeci c thalam ic nucleus is the centrom edian nucleus, which is doubtless certainly one of the intralam inar nuclei. It receives a erent f bers from the cerebellum, reticular kind ation, and m edial pallidus. Head of caudate nucleus Globus pallidus, m edial segm ent Globus pallidus, lateral segm ent Putam en Centrom edian nucleus Em boliform nucleus of cerebellum Mam m illary body Reticular kind ation of brainstem Mam m illothalam ic fasciculus 336 Neuroanatomy 14. Diencepha lon Ventral lateral nucleus Lateral posterior nucleus Globus pallidus, m edial segm ent Globus pallidus, lateral segm ent Lateral dorsal nucleus Dorsal m edial nucleus Putam en Medial geniculate physique Hypothalam us (afferent) Lateral geniculate body C Medial, posterior, and lateral thalamic nuclei: a erent and e erent connections the medial thalamic nuclei obtain their a erent input from ventral and intralam inar thalam ic nuclei (not shown), the hypothalam us, the m esencephalon, and the globus/pallidus. Their e erent bers project to the frontal lobe and prem otor cortex, and a erent bers from these regions return to the nuclei. The destruction of these tract s results in frontal lobe syndrome, which is characterized by a loss of self-control (episodes of childish jocularit y alternating with suspicion and petulance). The posterior nuclei are kind ed by the pulvinar, which is the most important nuclear complicated of the thalam us. The pulvinar receives a erent bers from different thalam ic nuclei, notably the intralam inar nuclei (not shown). Its e erent bers time period inate within the affiliation areas of the parietal and occipital lobes, which have reciprocal connections with the pulvinar. The lateral geniculate physique (part of the visible pathway) project s to the visible cortex, whereas the m edial geniculate physique (part of the auditory pathway) project s to the auditory cortex. The lateral nuclei include the lateral dorsal nucleus and lateral posterior nucleus. They symbolize the dorsal portion of the ventrolateral group and receive their enter from other thalam ic nuclei (hence the term "integration nuclei," see p. D Synopsis of some clinically important connections of the speci c thalamic nuclei the speci c thalam ic nuclei project to the cerebral cortex. The desk under lists the origins of the tracts that time period inate within the nuclei, the nuclei them selves, and the sites to which their a erent bers project. The hypothalam us is the lowest degree of the diencephalon, located below the thalam us. The hypothalam us is a sm all nuclear complex situated ventral to the thalam us and separated from it by the hypothalam ic sulcus. Despite its sm all size, the hypothalam us is the com m and center for all autonom ic capabilities within the body. The Term inologia Anatom ica lists over 30 hypothalam ic nuclei located within the lateral wall and oor of the third ventricle. Only a couple of of the bigger, m ore clinically essential nuclei are m entioned on this unit. Three teams of nuclei are listed below in a rostral-to-caudal sequence, and their features are brie y described: � the anterior (rostral) group of nuclei (green) synthesizes the horm ones launched from the posterior lobe of the pituitary gland, and consist s of the � preoptic nucleus, � paraventricular nucleus, and � supraoptic nucleus. It consist s of the � posterior nucleus and � m am m illary nuclei positioned within the m am m illary our bodies. The coronal section (c) exhibits the additional subdivision of the hypothalam us by the fornix into lateral and m edial zones. Bilateral lesions of the m am m illary bodies and their nuclei are m anifested by the K orsako syndrome, which is frequently associated with alcoholism (cause: vitam in B1 [thiam ine] de ciency). A m ajor neuropathological nding is the presence of hem orrhages within the m am m illary our bodies, which are sectioned at autopsy to con rm the diagnosis. Diencepha lon Stria term inalis Fornix To reticular form ation Mam m illothalam ic fasciculus Stria m edullaris thalam i Posterior nucleus Medial forebrain bundle Preoptic nucleus Supraoptic nucleus Amygdala Paraventricular nucleus Supraoptic nucleus Tuberohypophyseal tract Hypothalam ichypophyseal tract Posterior lobe of pituitary gland a Hippocam pus Mam m illary physique Peduncle of mam m illary body b Retroflex tract Mam m illotegm ental tract Dorsal longitudinal fasciculus C Important a erent and e erent connections of the hypothalamus Midsaggital section of the best hem isphere considered from the m edial aspect. Because the hypothalam us coordinates all of the autonom ic functions in the physique, it establishes a erent (blue) and e erent (red) connections with m any brain regions. The bers of this tract m ediate the change of autonom ic inform ation wager ween the hypothalam us, cranial nerve nuclei, and spinal twine. D Functions of the hypothalamus the hypothalam us is the coordinating center of the autonom ic nervous system. Certain capabilities may be assigned to speci c regions or nuclei within the hypothalam us, and these relationships are outlined in the desk. Region or nucleus Function Anterior preoptic region Maintains constant physique temperature; Lesion: central hypothermia Responds to temperature modifications. The pituitary gland (hypophysis) consists of t wo lobes: � Anterior lobe (adenohypophysis), which is a horm one-producing and releasing part (see D and E), and � Posterior lobe (neurohypophysis), which is a horm one-releasing half for horm ones produced in the hypothalam us. While the posterior pituitary lobe is an extension of the diencephalon, the anterior pituitary lobe is derived from the epithelium of the roof of the pharynx. The pituitary stalk (infundibulum) at taches both lobes of the gland to the hypothalam us. The peptide horm ones are stored in vesicles (aggregated into massive "Herring our bodies") within the cell bodies of the neurosecretory neurons and are carried to the posterior lobe by anterograde axoplasm ic transport. Diencepha lon Dorsom edial nucleus C Hypophyseal portal circulation and connections of the hypothalamic nuclei to the anterior pituitary lobe the superior hypophyseal arteries from each side of the physique form a vascular plexus across the infundibulum (pituitary stalk). The axons from neurons of the hypothalam ic nuclei (dark pink and darkish blue arrows) time period inate at this plexus and secrete horm ones that have been produced in sm aller (parvocellular) neurons of the hypothalam us. The secreted hypothalam ic horm ones are of t wo t ypes: � Releasing elements which stim ulate horm one release from cells of the anterior pituitary lobe � Inhibiting factors which inhibit the horm onal release from these cells these horm ones are carried by the hypophyseal (pituitary) portal venous system (nam ed after the portal circulation of the liver) to capillaries in the anterior lobe, establishing com m unication guess ween the hypothalam us and endocrine cells of the anterior pituitary.
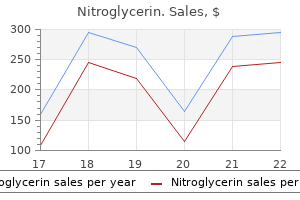
Quality nitroglycerin 6.5 mgThe highest point on the plot is the last word (tensile) stress medicine rock nitroglycerin 2.5 mg buy generic on-line, and is indicative of the energy of the material symptoms viral infection nitroglycerin 2.5 mg free shipping. The graph then slopes downwards as necking of the pattern occurs earlier than last failure. The space under the graph signifies the amount of power absorbed before failure and is a measure of the toughness of the fabric. The y-axis is the stress and the x-axis is the variety of cyclical loadings, often on a logarithmic scale. In orthopaedic functions up to 10 million cycles are usually used for the x-axis. A S�N curve usually follows an exponential downward shape, flattening off in path of a horizontal line at the right side of the curve. The endurance limit is a line drawn tangential to the horizontal part of the curve and marks the stress at which the fabric might theoretically be loaded an infinite variety of times with out failing. The point at which the curve starts on the y-axis is identical as the ultimate word tensile stress of the fabric, i. Titanium, for instance, is notch delicate and fails far more simply if there are defects on its surface. Stainless steel is topic to crevice crack corrosion, which makes it extra susceptible to fatigue failure over time when in vivo. The form of any implant is also very important in defining its mechanical properties. Other indications would include peripheral vascular disease, an infection, tumours, nerve harm (trophic ulceration), and congenital anomalies. It is crucial to retain a most degree of unbiased function whilst removing all diseased tissue, and minimizing morbidity and mortality. The amputation must be thought of to be the preliminary stage of a reconstruction procedure aiming to produce a physiological finish organ, and as such a multidisciplinary strategy is required if I am to achieve success in returning the patient to maximal perform. In the elective setting, after taking a radical historical past, I would assess the tissues clinically-feeling pulses and pores and skin temperature. I would use a Doppler ultrasound in search of an ankle�brachial index of greater than zero. I would like the patient to have a serum albumin of a minimal of three g/dl and a white cell count of greater than 1500/ml. I would purpose for pre-operative management of diabetes, consider cardiac, renal, and cerebral circulation, and supply dietary help for a malnourished affected person. As important as scientific evaluation is pre-operative psychological counselling and input from the ache staff. In the trauma or acute setting not all of that is always potential, however I would still attempt to achieve as much of this as I can. I prefer to use a skew flap so as to move the skin incisions away from any areas that bear weight. I favor to use a tourniquet and divide pores and skin, subcutaneous fats, and fascia in the identical line as the periosteum of the anteromedial surface of the tibia. I elevate flaps to the extent of the amputation and work through every muscle compartment systematically. I identify the superficial peroneal nerve between extensor digitorum longus and peroneus brevis, pull it distally, and divide under tension. Then I divide the anterior tibial vessels and deep peroneal nerve and part anterior muscles 1�2 cm distal of the bony resection. Now the anterior and lateral compartments are prepared, I can section the tibia and bevel the tip, and then section the fibula three cm proximal to the tibia. In the posterior compartment I should divide the posterior vessels and nerve and trend a posterior flap which can involve thinning of the muscle bulk and bevelling the muscular tissues. I would then release the tourniquet and procure haemostasis, and shut the wound in layers over a drain. I choose a delicate dressing for the residuum, and ideally this is taken down inside 48 hours. Any dressings which are used should keep away from proximal compression as they danger performing like a venous tourniquet. As quickly because the wound is healed, pomade can start, which is the method of therapeutic massage to scale back swelling. Pain may also be a result of a pointy bony prominence-a failure to bevel the bone ends or leave enough muscle to cowl them adequately. The T-score is the number of commonplace deviations below the mean compared with a raceand sex-matched adult population (25�35-year-olds). The Z-score is the variety of commonplace deviations below the imply for an age-, race-, and sex-matched adult population. Possible unwanted effects of alendronate include upper gastrointestinal disturbance, irregular taste, muscle and joint pain, dizziness, rash, osteonecrosis of the jaw, and subtrochanteric femoral fractures. A 12 months after beginning therapy this affected person presents with a further fracture of her wrist after a fall. Alendronate, etidronate, risedronate, raloxifene and strontium ranelate for the primary prevention of osteoporotic fragility fractures in postmenopausal women (amended). Alendronate, etidronate, risedronate, raloxifene, strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women (amended). They have an easily identifiable color code for placing patients right into a triage bracket depending on the severity of their accidents, and likewise establish the potential for contamination, for example in a chemical spill. Triage is the process of prioritizing affected person remedy during mass-casualty events. The central tenet is that you must do the most good for the most patients utilizing the obtainable resources. In mass-casualty (as against multiple-casualty) occasions the need is larger than the assets obtainable. This will end in delays to evacuation to definitive care and variation in the standard of care achieved-at least initially. Careful command and control with dispersal of casualties to a number of hospitals is intended to avoid overwhelming a single facility. Patients with airway issues are triaged ahead of these with breathing problems, circulatory issues, or incapacity. It is necessary that those patients with unsurvivable accidents are recognized rapidly to avoid consuming sources in the course of the time of triage. In the worst-case scenario, resources that could have saved a number of other casualties are depleted during makes an attempt to save a single critically injured casualty whose possibilities of survival were always exceedingly remote. Triage officers are deployed to the scene of an incident, and are again situated just exterior the emergency department of a receiving hospital and likewise throughout the pre-operative area of a theatre complicated.
Buy 2.5 mg nitroglycerin with amexNote: the visceral e erent symptoms weight loss purchase 2.5 mg nitroglycerin with visa, parasympathetic nuclear complicated (visceral oculom otor [Edinger-Westphal] nucleus) can be distinguished from the som atic e erent nuclear complex (nucleus of the oculom otor nerve) medicine holder nitroglycerin 6.5 mg amex. The nuclei of the oculom otor nerve and trochlear nerve are located within the m idbrain (m esencephalon), whereas the nucleus of the abducent nerve is located within the pons. Course: the trochlear nerve em erges from the posterior floor of the brainstem close to the m idline, courses anteriorly across the cerebral peduncle, and enters the orbit by way of the superior orbital ssure. Special features: � the trochlear nerve is the only cranial nerve in which all of the bers cross to the other facet (see A). Consequently, lesions of the nucleus or of nerve bers very close to the nucleus, before they cross the m idline, result in trochlear nerve palsy on the aspect opposite to the lesion (contralateral palsy). A lesion previous the location where the nerve crosses the midline results in trochlear nerve palsy on the sam e side as the lesion (ipsilateral palsy). Nucleus and distribution: the nucleus of the trochlear nerve is positioned in the m idbrain (m esencephalon). Its e erents provide m otor innervation to one extraocular m uscle, the superior indirect. E ects of trochlear nerve harm: � the a ected eye is greater and can also be deviated medially because the inferior indirect (responsible for elevation and abduction) becom es dom inant due to loss of the superior oblique. Course: the nerve runs anteriorly from the m esencephalon (m idbrain = highest degree of the brainstem; see pp. Course: the nerve follows a long extradural path earlier than entering the orbit by way of the superior orbital ssure. Nucleus and distribution: � the nucleus of the abducent nerve is situated in the pons (= midlevel brainstem), its bers emerging on the inferior border of the pons. All three cranial nerves extend from the brainstem through the superior orbital ssure into the orbit. Because of this, abducent nerve palsy m ay develop in association with m eningitis and subarachnoid hem orrhage. The oculomotor nerve provides parasym pathetic innervation to intraocular m uscles (it s parasympathetic bers synapse in the ciliary ganglion) as properly as som atic m otor innervation to m ost of the extraocular m uscles and the levator palpebrae superioris. Oculom otor nerve palsy m ay a ect the parasympathetic bers solely, the som atic m otor bers completely, or both on the sam e tim e (see B). Their peripheral bers innervate the facial pores and skin, giant portions of the nasopharyngeal mucosa, and the anterior t wo-thirds of the tongue (som atic sensation, see C). Clinical problems of the trigeminal nerve: Sensory disturbances and de cits could come up in various conditions: � Sensory loss as a end result of traum atic nerve lesions. The larger sensory nuclei of the trigem inal nerve are distributed along the brainstem and prolong downward into the spinal twine. The sensory root (m ajor part) of the trigem inal nerve type s the bulk of the bers, whereas the motor root (m inor part) is kind ed by bers arising from the sm all m otor nucleus in the pons. The following somatic a erent nuclei are distinguished: � Mesencephalic nucleus of the trigeminal nerve: proprioceptive bers from the m uscles of m astication. Special function: the neurons of this nucleus are pseudounipolar ganglion cells that have m igrated into the brain. A sm all, circum scribed lesion of the trigem inal spinal sensory nucleus results in attribute sensory disturbances within the face (see D). The three divisions of the trigem inal nerve and clinically im portant time period inal branches are proven. All three divisions of the trigem inal nerve supply the skin of the face (b) and the m ucosa of the nasopharynx (c). The m uscles of m astication are supplied by the m otor root of the trigem inal nerve, whose axons enter the m andibular division (e). Their pat tern indicates the corresponding portion of the trigem inal nucleus during which the lesion is located (m atching color shades). The rst sm all branch arising from the ophthalmic division is the recurrent meningeal department, which provides sensory innervation to the dura m ater. The bulk of the ophthalm ic division bers enter the orbit from the m iddle cranial fossa by passing through the superior orbital ssure. The ophthalmic division divides into three branches the nam es of which point out their distribution: the lacrimal nerve, frontal nerve, and nasociliary nerve. Sympathetic bers accompany the long ciliary nerves that arise from the nasociliary nerve, traveling in these nerves to the pupil. Sensory bers from the eyeball course within the nasociliary root, passing by way of the ciliary ganglion to the nasociliary nerve. Its t wo time period inal branches, the zygom aticofacial branch and zygom ati- cotemporal department (not shown here), supply sensory innervation to the skin over the zygom atic arch and tem ple. Parasympathetic, submit synaptic bers from the pterygopalatine ganglion are carried to the lacrim al nerve by the com m unicating department (see p. The infraorbital nerve also passes via the inferior orbital ssure into the orbit, from which it enters the infraorbital canal. Its ne term inal branches provide the pores and skin bet ween the lower eyelid and higher lip. The m ixed a erent-e erent m andibular division leaves the m iddle cranial fossa through the foram en ovale and enters the infratemporal fossa on the external facet of the base of the skull. It s sensory branches are as follows: � � � � Auriculotemporal nerve Lingual nerve Inferior alveolar nerve (also carries m otor bers, see below) Buccal nerve travel with it. The a erent bers of the inferior alveolar nerve move by way of the m andibular foram en into the m andibular canal, the place they give o inferior dental branches to the m andibular enamel. The m ental nerve is a time period inal department that provides the skin of the chin, lower lip, and the body of the m andible. The e erent bers that department from the inferior alveolar nerve provide the mylohyoid m uscle and the anterior stomach of the digastric (not shown). The buccal nerve pierces the buccinator m uscle and supplies sensory innervation to the m ucous m em brane of the cheek. The pure motor branches go away the m ain nerve trunk just distal to the origin of the m eningeal branch. They are: � � � � � Masseteric nerve (m asseter m uscle) Deep temporal nerves (temporalis m uscle) Pterygoid nerves (pterygoid m uscles) Nerve of the tensor t ympani m uscle Nerve of the tensor veli palatini m uscle (not shown) the branches of the auriculotemporal nerve supply the tem poral pores and skin, the exterior auditory canal, and the t ympanic m em brane. The lingual nerve supplies sensory bers to the anterior t wo-thirds of the tongue, and gustatory bers from the chorda t ympani (facial nerve branch) V1 D Clinical assessment of trigeminal nerve perform Each of the three m ain divisions of the trigem inal nerve is examined separately during the physical exam ination. This is finished by pressing on the nerve exit factors with one nger to take a look at the feeling there (local tenderness to pressure). The other visceral e erent (parasympathetic) bers from the superior salivatory nucleus are grouped with the visceral a erent (gustatory) bers from the nucleus of the solitary tract to form the nervus intermedius and combination with the visceral e erent bers from the facial nerve nucleus. Sites of emergence: the facial nerve em erges within the cerebellopontine angle wager ween the pons and olive. It exit s the cranial cavit y via the interior acoustic m eatus passing into the petrous part of the temporal bone, the place it divides into its branches: � the special visceral e erent bers move by way of the stylomastoid foramen to exit the bottom of the skull to form the intraparotid plexus (see C, exception: stapedius n.
2.5 mg nitroglycerin order fast deliveryInternal cerebral vein Great cerebral vein Straight sinus Confluence of the sinuses Inferior anastom otic vein (of Labb�) Inferior petrosal sinus Transverse sinus Superior jugular bulb Superficial m iddle cerebral vein Anterior intercavernous sinus Cavernous sinus Parietal em issary vein Superior sagit tal sinus Straight sinus Superior petrosal sinus Occipital em issary vein Occipital vein Confluence of the sinuses Posterior auricular vein Sigm oid sinus Mastoid em issary vein Condylar em issary vein Deep cervical vein Inferior sagit tal sinus Basilar vein Frontal vein Superior ophthalm ic vein Angular vein Inferior ophthalm ic vein Cavernous sinus Venous plexus of foram en ovale Pterygoid plexus Inferior petrosal sinus Retrom andibular vein Facial vein Vertebral vein External jugular vein Internal jugular vein B Accessory drainage pathw ays of the dural sinuses Right lateral view symptoms to diagnosis nitroglycerin 2.5 mg purchase online. The dural sinuses have many accessory drainage pathways in addition to their principal drainage into the t wo inner jugular veins treatment alternatives cheap 6.5 mg nitroglycerin with mastercard. The connections wager ween the dural sinuses and extracranial veins primarily serve to equalize stress and regulate temperature. These anastom oses are of medical interest as a end result of their norm al path of blood ow may reverse (no venous valves), permitting blood from extracranial veins to re ux into the dural sinuses. This m echanism m ay give rise to sinus infections that lead, in turn, to vascular occlusion (venous si- nus thrombosis). The m ost essential accessory drainage vessels embody the following: � Em issary veins (diploic and superior scalp veins), see C � Superior ophthalm ic vein (angular and facial veins) � Venous plexus of foram en ovale (pterygoid plexus, retrom andibular vein) � Marginal sinus and basilar plexus (internal and external vertebral venous plexus), see C 374 Neuroa natomy 17. Blood Vessels of the Bra in Sagit tal suture Parietal foram en Parietal em issary vein Superior sagit tal sinus Lam bdoid suture Confluence of the sinuses Transverse sinus External occipital protuberance Sigm oid sinus Mastoid em issary vein Condylar canal Parietom astoid suture Occipital foram en Occipital em issary vein Mastoid foram en Venous plexus across the foram en m agnum (m arginal sinus) Mastoid process Venous plexus of hypoglossal nerve canal External vertebral venous plexus Condylar em issary vein Occipital condyle Internal jugular vein Occipital vein C Occipital emissary veins Em issary veins set up a direct connection wager ween the intracranial dural sinuses and extracranial veins. They run through sm all cranial openings such because the parietal and m astoid foram ina. Em issary veins are of clinical curiosity because they create a potential route by which micro organism from the scalp m ay unfold to the dura m ater and dural venous sinuses. The deep veins drain blood from the deeper portions of the white m at ter, basal ganglia, corpus callosum, and diencephalon into the great cerebral vein, which enters the straight sinus. The t wo venous regions (those of the tremendous cial and deep veins) are interconnected by num erous intracerebral anastom oses (see D). While the entire cerebral arteries enter the mind at it s base, venous blood is drained from the entire floor of the brain, together with the bottom, and in addition from the inside of the brain by t wo teams of veins: the superf cial cerebral veins and the deep cerebral veins. The super cial veins drain blood from the cerebral cortex (via cortical veins) and white m at- Superior cerebral veins Superior anastom otic vein (of Trolard) Superior sagit tal sinus Superficial m iddle cerebral vein a Inferior anastom otic vein (of Labb�) Anterior vein of septum pellucidum Thalam ostriate vein Superior cerebral veins Inferior sagit tal sinus Choroid plexus of fourth ventricle Superior sagit tal sinus Great cerebral vein Internal occipital vein Inferior cerebral vein Anterior cerebral vein Internal cerebral vein Basilar vein b Occipital sinus Straight sinus Transverse sinus A Super cial veins of the mind (super cial cerebral veins) Left lateral view (a) and m edial view (b). Just earlier than time period inating in the dural sinuses, the veins leave the subarachnoid house and run a short subdural course guess ween the dura m ater and arachnoid. The bridging veins have great scientific importance as a outcome of they m ay be ruptured by head traum a, resulting in a subdural hem atom a (see p. The veins on the lateral surface of the brain are classi ed by their path of drainage as ascending (draining into the superior sagit tal sinus) or descending (draining into the transverse sinus). The tremendous cial m iddle cerebral vein drains into both the cavernous and transverse sinuses (see A, p. Olfactory nerve Anterior com m unicating vein Optic tract Interpeduncular vein Inferior choroidal vein Basilar vein Superficial m iddle cerebral vein Anterior cerebral vein Deep m iddle cerebral vein Cerebral peduncle Internal cerebral vein Great cerebral vein Posterior venous confluence C Basal cerebral venous system the basal cerebral venous system drains blood from each super cial and deep cerebral veins. A venous circle form ed by the basilar veins (of Rosenthal, see below) exist s on the base of the brain, analogous to the arterial circle of Willis. The basilar vein is form ed in the anterior perforate substance by the union of the anterior cerebral and deep m iddle cerebral veins. Following the course of the optic tract, the basilar vein runs posteriorly around the cerebral peduncle and unites with the basilar vein from the alternative side on the dorsal facet of the mesencephalon. The t wo internal cerebral veins also term inate at this venous junction, the posterior venous con uence. This junction gives rise to the m idline great cerebral vein, which enters the straight sinus. The t wo anterior cerebral veins are interconnected by the anterior com m unicating vein, making a closed, ringshaped drainage system. Superior sagit tal sinus Superficial cerebral veins Medullary anastom otic vein Superficial cerebral veins Medullary vein Longitudinal vein of caudate nucleus Transverse veins of caudate nucleus Choroidal vein Internal cerebral vein Term inal vein Deep m iddle cerebral vein Inferior lenticular veins Vein of centrum sem iovale Superficial m iddle cerebral vein Lateral superior lenticular veins Medial superior lenticular veins D Anastomoses betw een the tremendous cial and deep cerebral veins Transverse part through the left hem isphere, anterior view. The super cial cerebral veins com m unicate with the deep cerebral veins through the anastom oses proven here (see p. Flow reversal (double arrows) may happen in the boundary zones bet ween t wo territories. The temporal and occipital lobes and tentorium cerebelli have been rem oved on the left aspect to dem onstrate the upper floor of the cerebellum and the superior cerebellar veins. On the lateral walls of the anterior horns of each lateral ventricles, the superior thalam ostriate vein runs towards the interventricular foram en in the groove guess ween the thalam us and caudate nucleus. After receiving the anterior vein of the septum pellucidum and the superior choroidal vein, it form s the interior cerebral vein and passes through the interventricular foram en along the roof of the diencephalon toward the quadrigem inal plate, which incorporates the superior and inferior colliculi. There it unites with the interior cerebral vein of the alternative side, and the basal veins to kind the posterior venous con uence, which supplies rise to the nice cerebral vein. Veins of caudate nucleus Anterior vein of septum pellucidum Internal cerebral vein Basal vein Posterior vein of corpus callosum Interventricular foram en Superior thalam ostriate vein Superior choroidal vein Lateral vein of lateral ventricle Great cerebral vein Medial vein of lateral ventricle Straight sinus Superior cerebellar veins Confluence of the sinuses Quadrigem inal plate Inferior petrosal sinus Petrosal vein Sigm oid sinus Great cerebral vein Superior vein of verm is Superior petrosal sinus Verm is (Lateral) inferior cerebellar vein (Lateral) superior cerebellar vein (Medial) superior cerebellar vein Transverse sinus Straight sinus (Medial) inferior cerebellar vein Confluence of the sinuses Inferior vein of verm is B Cerebellar veins Posterior view. Like the opposite veins of the brain, the cerebellar veins are distributed independently of the cerebellar arteries. Larger trunks cross over gyri and sulci, running m ainly within the sagit tal course. A medial and a lateral group can be distinguished based on their gross topographical anatomy. The m edial group of cerebellar veins drains the verm is and adjoining parts of the cerebellar hem ispheres (precentral vein, superior and inferior veins of the verm is) and the m edial parts of the superior and inferior cerebellar veins. The lateral group (petrosal vein and lateral portions of the superior and inferior cerebellar veins) drains m ost of the t wo cerebellar hem ispheres. All of the cerebellar veins anastom ose with each other; their out ow is exclusively infratentorial. Blood Vessels of the Bra in Internal cerebral vein Inferior sagit tal sinus Thalam ostriate vein Anterom edial anastom osis Anterolateral anastom osis Trigem inal nerve Anterom edian pontine vein Transverse pontine veins Interpeduncular veins Pontom esencephalic vein Superior verm ian vein Superior cerebellar veins Anterolateral pontine vein Basal vein C Reg ion drained by the deep cerebral veins Coronal section. Three principal venous segm ents could be identi ed in each hem isphere: � Thalam ostriate vein � Internal cerebral vein � Basal vein the region drained by the deep cerebral veins encompasses massive portions of the bottom of the cerebrum, the basal ganglia, the inner capsule, the choroid plexuses of the lateral and third ventricles, the corpus callosum, and portions of the diencephalon and m esencephalon. Transverse m edullary veins a Posterom edian m edullary vein Posterior choroidal vein Internal cerebral veins D Veins of the brainstem a Anterior view of the brainstem in situ (the cerebellum and part of the occipital lobe have been rem oved on the left side). The veins of the brainstem are a continuation of the veins of the spinal wire and join them with the basal veins of the mind. The veins of the m edulla oblongata, pons, and cerebellum m ake up the infratentorial venous system. Great cerebral vein Superior cerebellar vein Trigem inal nerve Superior petrosal vein Accessory basal vein Trochlear nerve Variant of basal vein Lateral m esencephalic vein Lateral m edullary vein Posterolateral medullary vein Dorsal transverse m edullary veins b Posterom edian m edullary vein Caudal cerebellar peduncular vein Vein of cerebellom edullary cistern 379 Neuroanatomy 17. A Extracerebral hemorrhages Extracerebral hem orrhages are de ned as bleeding bet ween the calvaria and mind. Because the bony calvaria is im m obile, the creating hem atom a exert s strain on the delicate brain. Depending on the supply of the hem orrhage (arterial or venous), this m ay produce a rapidly or slowly creating incompressible m ass with a rise of intracranial pressure that m ay dam age not only the brain tissue on the bleeding web site but in addition in m ore rem ote brain areas. Three t ypes of intracranial hem orrhage may be distinguished primarily based on their relationship to the dura m ater: a Epidural hematoma (epidural = above the dura). The bleeding m ost com m solely occurs from a ruptured m iddle m eningeal artery (due to the shut proxim it y of the m iddle m eningeal artery to the calvaria, a sharp bone fragm ent m ay lacerate the artery). The hem atom a form s guess ween the calvaria and the periosteal layer of the dura m ater. Pressure from the hem atom a separates the dura from the calvaria and displaces the mind.
Buy 6.5 mg nitroglycerin with mastercardLike the Golgi equipment symptoms thyroid cancer trusted 6.5 mg nitroglycerin, endosomes are concerned in sorting treatment definition math discount nitroglycerin 6.5 mg without prescription, modifying, and directing vesicular site visitors in cells. Associated with this organelle, significantly close to its concave floor, are a number of roughly spherical, membrane-enclosed vesicles. Proteins arriving on the Golgi apparatus from the tough endoplasmic reticulum endure a series of modifications as they pass from one Golgi compartment to the next. For instance, carbohydrates are linked to proteins to kind glycoproteins, and the length of the protein is usually shortened by removing a terminal portion of the polypeptide chain. Portion of mitochondrion Rough endoplasmic reticulum Rough endoplasmic reticulum Structure: Extensive membranous community of flattened sacs. The outer membrane is clean, whereas the inside membrane is folded into sheets or tubules often identified as cristae, which lengthen into the inner mitochondrial compartment, the matrix. Large numbers of them, as many as a thousand, are current in cells that make the most of massive amounts of power, whereas less energetic cells contain fewer. Our fashionable understanding of mitochondrial construction and function has developed, however, from the thought that every mitochondrion is bodily and functionally isolated from others. This interconnected community of mitochondria may be particularly essential in the distribution of oxygen and energy sources (notably, fatty acids) throughout the mitochondria inside a cell. Moreover, the extent of the reticulum might change in different physiological settings; extra mitochondria could fuse, or split apart, and even destroy themselves because the energetic demands of cells change. In addition to providing a lot of the vitality required to power physiological occasions similar to muscle contraction, mitochondria also operate within the synthesis of sure lipids, such as the hormones estrogen and testosterone (Chapter 11). The fluid inside a lysosome is acidic and accommodates a wide range of digestive enzymes. Lysosomes act to break down micro organism and the debris from lifeless cells that have been engulfed by Cellular Structure, Proteins, and Metabolic Pathways 53 Membrane-enclosed vesicle Golgi equipment Structure: Series of cup-shaped, carefully apposed, flattened, membranous sacs; associated with quite a few vesicles. Generally, a single Golgi apparatus is positioned in the central portion of a cell close to its nucleus. Function: Concentrates, modifies, and kinds proteins arriving from the rough endoplasmic reticulum prior to their distribution, by means of the Golgi vesicles, to other organelles or to secretion from the cell. They can also break down cell organelles which were broken and now not operate normally. They have an especially important perform within the varied cells that make up the defense techniques of the body (Chapter 18). Hydrogen peroxide may be toxic to cells in high concentrations, but peroxisomes can even destroy hydrogen peroxide and thereby prevent its poisonous results. Peroxisomes Like lysosomes, peroxisomes are reasonably dense oval bodies enclosed by a single membrane. Like mitochondria, peroxisomes devour molecular oxygen, though in much smaller quantities. These tiny constructions have been described as barrel-shaped but additionally as resembling Cristae (inner membrane) Matrix Outer membrane Mitochondrion Structure: Rod- or oval-shaped body surrounded by two membranes. The mitochondria are indicated by the letter m; different labels check with buildings found in skeletal muscle and might be described in later chapters. This has led to the hypothesis that vaults are important for transport of molecules between the cytosol and the nucleus. For instance, elevated expression of this vault protein has been linked in some research to drug resistance, together with some drugs used in the treatment of most cancers. If true, then vaults might someday present a target for modulating the effectiveness of such drugs in human patients. Cytoskeleton In addition to the membrane-enclosed organelles, the cytoplasm of most cells accommodates quite lots of protein filaments. The three lessons of cytoskeletal filaments are based on their diameter and the kinds of protein they include. Actin filaments and microtubules may be assembled and disassembled quickly, permitting a cell to alter these elements of its cytoskeletal framework according to altering requirements. In distinction, intermediate filaments, as quickly as assembled, are less readily disassembled. Actin filaments are composed of monomers of the protein G-actin (or "globular actin"), which assemble right into a polymer of two twisting chains generally identified as F-actin (for "filamentous"). They have important functions in figuring out cell shape, the ability of cells to transfer by amoeboid-like movements, cell division, and muscle cell contraction. Intermediate filaments are composed of twisted strands of several totally different proteins, including keratin, desmin, and lamin. They provide considerable strength to cells and consequently are most extensively developed in the areas of cells topic to mechanical stress (for instance, in association with desmosomes). Microtubules are hollow tubes about 25 nm in diameter, whose subunits are composed of the protein tubulin. Microtubules additionally radiate from a area of the cell generally recognized as the centrosome, which surrounds two small, cylindrical our bodies known as centrioles, composed of nine units of fused microtubules. The centrosome is a cloud of amorphous materials that regulates the formation and elongation of microtubules. During cell division, the centrosome generates the microtubular spindle fibers used in chromosome separation. Microtubules and actin filaments have also been implicated within the movements of organelles inside the cytoplasm. These fibrous elements type tracks, and organelles are propelled along these tracks by contractile proteins connected to the surface of the organelles. Cellular Structure, Proteins, and Metabolic Pathways fifty five Cilia, the hairlike extensions on the surfaces of most cells, have a central core of microtubules organized in a pattern much like that discovered in the centrioles. In motile cilia, typically situated on certain epithelial cells, the microtubules, in combination with a contractile protein, produce actions of the cilia. In hole organs lined with ciliated epithelium, the actions of the cilia assist propel the contents of the organ alongside the surface of the epithelium. An example of that is the cilia-mediated motion of mucus in opposition to gravity up the trachea, which helps take away inhaled particles that would injury the lungs. The other sort of cilium is identified as a nonmotile, or major, cilium; most eukaryotic cells have one or a small number of nonmotile cilia. Physiologists have identified a lot of ailments related to mutated genes expressed in cilia in several tissues; collectively, these illnesses are often known as ciliopathies and happen most incessantly in the retina, liver, kidneys, and brain. The endoplasmic reticulum is a community of flattened sacs and tubules within the cytoplasm. Rough endoplasmic reticulum has hooked up ribosomes and is primarily involved in the packaging of proteins to be secreted by the cell or distributed to different organelles. Smooth endoplasmic reticulum is tubular, lacks ribosomes, and is the site of lipid synthesis and calcium accumulation and release. The Golgi equipment modifies and sorts the proteins that are synthesized on the rough or granular endoplasmic reticulum and packages them into secretory vesicles. Endosomes are membrane-bound vesicles that fuse with vesicles derived from the plasma membrane and bud off vesicles that travel to other cell organelles.
Syndromes - Colic in infants
- Thoracentesis--removing fluid from the space between the outside lining of the lungs and the chest wall
- Abdominal MRI
- Blood gases
- Iron deficiency
- Label the container with your name, the date, the time of completion, and return it as instructed.
- Use of drugs that are toxic to the liver
- Never leave infants and children unattended in a bathtub.
- Pelvic pain during intercourse
- Take the drugs your doctor told you to take with a small sip of water.
Nitroglycerin 6.5 mg generic with amexSurgical debridement and excision of these structures might mitigate ache by limiting the quantity of residual free nerve-ending tissue symptoms hypothyroidism discount nitroglycerin 2.5 mg with visa, improving long-term surgical outcomes symptoms quotes order 2.5 mg nitroglycerin. This totally arthroscopic technique permits complete resection of the biceps proximal fragment along with the transverse ligament and the tendon sheath. The space is well-vascularized by the ascending department of the anterior circumflex artery. However, fixing the tendon into a bone socket with an interference screw seems the most suitable choice to achieve faster therapeutic and a shorter rehabilitation period. The patient is holding her arm with 10 levels of inner rotation and refers extreme pain when the examiner applies pinpoint pressure at the bicipital groove. The affected person complains of pain on the bicipital groove with the forearm in supination and downward resistance towards shoulder flexion. The patient complains of pain at the bicipital groove during resisted arm flexion with 30 degrees of arm adduction and the forearm in full pronation. Equipment this procedure requires commonplace arthroscopic tools with a 30-degree view arthroscope (Table 14-1). However, a specially designed cannula (PassPort Button Cannula [Arthrex]) can be useful for deltoid retraction, and an eight. Mainly 2 totally different methods are utilized to fix the biceps tenodesis at the suprapectoral area with interference screws. Increased up to 50 mm Hg during surgery based on blood strain and visualization. Suture and tissue management Coagulation and tissue vaporization Prevent tendon spinning Deltoid retraction to improve room and visualization Standard shoulder instruments set Radiofrequency gadget Cannula 8. Positioning and Portals the beach chair place is most well-liked for any sort of anterior shoulder extra-articular process because the patient can tolerate the process with solely a plexus block, and the anatomic landmarks are easier acknowledged and 3D surgical orientation is less demanding. This position allows simpler control of shoulder and elbow flexion and rotation during surgery. Furthermore, the fact that the scope is positioned at the lateral portal through the massive a part of the process additional emphasizes the benefit of utilizing the seashore chair over the lateral decubitus place. During surgery, sufferers receive an intravenous infusion of propofol, titrated to achieve light sleep. For optimum surgical visualization, intraoperative systolic blood strain is maintained at about a hundred and ten mm Hg. For safety reasons, the authors recommend measuring regional mind oxygen saturation with disposable scalp transducers. Step-by-Step Description of the Procedure Step 1: Portals and Tendon Evaluation the whole scapula and arm are prepped and draped to allow unrestricted access to the anterior and posterior shoulder buildings. This portal is located 2 cm distal and a pair of cm medial to the posterolateral nook of the acromion. The lateral portal is created between the middle and anterior third of the humeral head, 3 cm lateral from the acromion lateral edge. The shoulder is held in 30 levels of flexion, approximately 10 degrees of inside rotation, and 30 levels of abduction, permitting distension of the subacromial bursa and making certain a clear view of the bicipital groove. With the scope on the posterior portal and a probe by way of the anterosuperior portal, a radical inspection of the glenohumeral joint is made. The transverse ligament and the roof of the bicipital groove had been detached with a radiofrequency device. Dissection requires particular care due to the proximity of these structures with the underlying tendon. Typically, this maneuver is carried out from proximal to distal up to the level of the falciform ligament at the upper a part of pectoralis major tendon. With a bullet tip reamer, the surgeon drills a 20-mm deep bone socket approximately 10 mm above the pectoralis main tendon. Typically, a 9-mm diameter tunnel is drilled for feminine sufferers and a 10-mm diameter tunnel is drilled for male patients. Illustration indicating the related anatomy for an arthroscopic biceps tenodesis. Step 4: Restoring the Correct Length-Tension Relation A major objective of the tenodesis procedure is to restore the conventional length-tension relation of the tendon. To get hold of a traditional length-tension relation, the buried segment should derive from the tendon proximal to the bone socket. By doing so, the authors stop steering of the distal tendon phase into the socket. Before tenotomy, the authors carry out a tag stitch via the tendon precisely at the stage of the cartilage rim. This surgical gesture holds the tendon after tenotomy and acts as a useful landmark for additional measurements. The imply tendon length from the level of the cartilage rim as much as the superior border of the pectoralis major tendon is roughly 50 to fifty five mm. Therefore, the space between the bone socket and the holding sew is 40 to forty five mm. A sizer can be utilized to take the measurements; however, any instrument can work for this task as a caliper. If the deliberate interference screw is 20-mm lengthy, then the forked tip should seize the tendon 20 to 25 mm above the socket level or approximately halfway between the superior edge of the pectoralis main tendon and the articular cartilage rim. Step 5: Tenotomy and Interference Screw Fixation After retrieving the sutures of the superior tag sew from the posterior portal, tenotomy is performed with radiofrequency proper before interference screw fixation. There are a selection of methods for biceps tenodesis out there; nevertheless, all of them share the same principles. Some implants have a polyetheretherketone forked tip as part of the insert to push the tendon inside the socket. In different gadgets, the fork is part of the devices and it comes out before screw fixation. By loading the sutures tails via the eyelets at the implant tip, the surgeon can simply steer the tendon inside the socket, acquiring an optimum length-tension relation. Use depth indicators on the distal finish of the tendon fork to make positive the tendon is absolutely seated into the socket. A trocar tipped information wire is positioned via the fork to hold the tendon into the socket. Strengthening and gradual return to sports are anticipated between three and 5 months after surgical procedure. Due to intraoperative bleeding and visualization issues, the procedure may require conversion to an open subpectoral tenodesis. At medium-term scientific follow-up (mean 14 months, vary 6 to 32 months), the authors observed fixation failure ("Popeye sign") in four circumstances (8. Furthermore, the open subpectoral tenodesis with distal fixation near a slim diaphysis has a larger risk of humeral fracture. To guarantee a pleasing surgery, place the affected person within the beach chair position, use the scope by way of the lateral portal, and create 2 anterior portals for introduction of surgical tools. All of the dissections and tissue removing must be accomplished with a radiofrequency system. Retract and maintain the tendon out of the groove with a switching stick and use the reamer in a precisely perpendicular fashion to the bone.
Buy nitroglycerin 2.5 mg without prescriptionFor instance symptoms 22 weeks pregnant nitroglycerin 2.5 mg order with visa, so long as the concentration of sodium ions in the blood stays within a number of share factors of its normal vary symptoms 3 days after embryo transfer cheap nitroglycerin 2.5 mg free shipping, Na1 homeostasis exists. However, an individual whose Na1 concentration is homeostatic may suffer from different disturbances, similar to an abnormally low pH in the blood resulting from kidney illness, a condition that might be deadly. Just one nonhomeostatic variable, among the many many that might be described, can have life-threatening penalties. Often, when one variable turns into significantly out of steadiness, other variables in the physique turn into nonhomeostatic as a consequence. For instance, when you train strenuously and start to get warm, you perspire, which helps preserve body temperature homeostasis. This is important, because many cells (notably neurons) malfunction at elevated temperatures. In general, if all the most important organ techniques are working in a homeostatic method, a person is in good well being. Certain kinds of illness, in fact, can be defined because the loss of homeostasis in one or more techniques in the body. Stability of an inside environmental variable is achieved by the balancing of inputs and outputs. In the earlier instance, the variable (body temperature) stays constant because metabolic heat production (input) equals warmth loss from the physique (output). Now think about that we quickly decrease the temperature of the room, say to 58C, and hold it there. Very rapidly, nevertheless, quite a lot of homeostatic responses occur to restrict the lower. The first homeostatic response is that blood vessels to the skin turn out to be constricted (narrowed), lowering the quantity of blood flowing by way of the skin. The compensating mechanisms that mediate such responses are performed by homeostatic control methods. This time, our topic is a resting, lightly clad man in a room having a temperature of 208C and reasonable humidity. However, the chemical reactions occurring within the cells of his physique are producing warmth at a rate equal to the rate of heat loss. Under these conditions, the physique undergoes no web gain or lack of heat, and the body temperature stays fixed. This flow diagram is typical of those used all through this book to illustrate homeostatic techniques, and several conventions ought to be noted. For example, decreased room temperature tends to trigger an increase in heat loss from the physique, and curling up tends to cause a lower in warmth loss from the body. Qualifying the connection in this way is critical as a result of variables like warmth production and heat loss are underneath the influence of many elements, some of which oppose each other. Like the person proven within the chapter-opening photo, our subject hunches his shoulders and folds his arms in order to reduce the floor space of the skin obtainable for heat loss. This helps somewhat, but heat loss still continues, and physique temperature keeps decreasing, though at a slower rate. Our topic begins to shiver, and the chemical reactions responsible for the skeletal muscle contractions that constitute shivering produce giant portions of warmth. Feedback Systems the thermoregulatory system simply described is an example of a adverse suggestions system, during which an increase or decrease within the variable being regulated brings about responses that tend to move the variable in the direction reverse ("negative" to) the direction of the unique change. Thus, in our instance, a decrease in body temperature led to responses that tended to increase the body temperature-that is, move it towards its unique worth. Without negative suggestions, oscillations like some of these described on this chapter can be a lot larger and, subsequently, the variability in a given system would improve. Negative feedback also prevents the compensatory responses to a lack of homeostasis from continuing unabated. Details of the mechanisms and traits of negative feedback in several systems shall be addressed in later chapters. For now, you will want to acknowledge that negative suggestions has a significant part in the checks and balances on most physiological variables. This may happen by several processes, similar to chemical modification of the enzyme by the product of the response. Normally, glucose molecules are enzymatically broken down inside cells to release some of the chemical energy that was contained within the bonds of the molecule. In some instances, positive suggestions accelerates a process, leading to an "explosive" system. This is counter to the overall physiological precept of homeostasis, as a end result of constructive suggestions has no apparent means of stopping. Not surprisingly, due to this fact, positive suggestions is far much less widespread in nature than unfavorable feedback. Nonetheless, there are examples in physiology by which constructive suggestions is very important. This self-perpetuating cycle continues until finally the baby pushes via the stretched cervix and is born. In addition, the set points for a lot of regulated variables may be physiologically reset to a new worth. The homeostatic management systems regulating body temperature are still functioning throughout a fever, but they preserve the temperature at an elevated worth. This regulated increase in physique temperature is adaptive for combating the infection, as a end result of elevated temperature inhibits proliferation of some pathogens. The set point for body temperature has been reset to a higher value, and the body responds by shivering to generate heat. By inhibiting the exercise of the primary enzyme involved within the formation of a product, the product can regulate the rate of its personal formation. For instance, the set level for physique temperature is greater during the day than at night. Although the resetting of a set point is adaptive in some cases, in others it merely reflects the clashing demands of different regulatory methods. In our earlier example, body temperature was maintained regardless of massive swings in ambient temperature, however solely as a result of the homeostatic management system led to massive changes in skin blood circulate and skeletal muscle contraction. This is what we imply by "clashing calls for," which explains the phenomenon talked about earlier in regards to the interaction between body temperature and water balance during exercise. One further level is that, as is illustrated by the regulation of body temperature, a quantity of techniques normally management a single parameter. The effect is to put together the digestive system for the arrival of meals earlier than we even devour it, for instance, by inducing saliva to be secreted in the mouth and causing the abdomen to churn and produce acid. In our examples, feedforward regulation makes use of a set of exterior or inner environmental detectors.
Order nitroglycerin 2.5 mg overnight deliveryMany animal viruses use the cell membranes to envelope their particles treatment for piles nitroglycerin 2.5 mg purchase mastercard, and this facilitates their entry into host cells medications causing dry mouth 6.5 mg nitroglycerin safe. Plant viruses very rarely have membrane envelopes, and the few that do are in all probability actually insect viruses that additionally replicate in vegetation. Plant viruses are confronted with a different challenge: the means to penetrate the plant cell walls. To enter the plant they usually use insects that feed on crops, but other creatures can even serve this function, including grazing animals, nematodes that colonize plant roots, and even fungi. These all serve as vectors that permit viruses to move between crops, that are largely immobile with the exception of their seeds. Other things can act as vectors for some plant viruses embody pruning shears, lawnmowers, and the physical dealing with of plant materials. If vectors remedy the issue of stepping into plant hosts, how do plant viruses then move between plant cells This protein adjustments the size of the small pores that join plant cells, and permits the viruses to move through. Some viruses transfer via these pores as intact virus particles, while others transfer as their naked genome. However, most virus-host trade of genes goes the other means, from viruses to their hosts. These are referred to as persistent viruses, as a end result of they stick with their plant hosts by way of many generations by seed transmission. We embody the descriptions of two of those viruses right here, Oryza sativa endornavirus and White clover cryptic virus. Another characteristic of plant viruses never seen in animal viruses involves the way they package deal their genomes. Many plant viruses with segmented genomes bundle every phase in its own virus particle. This allows them to have more advanced genomes with very simple virus particles, but it also implies that they must get all of the particles into a host in a single place to start a model new an infection. It was grown sporadically until the early twentieth century when there was a powerful push to use cassava as an important staple food. By the Nineteen Twenties, reports of a severe mosaic disease in cassava became widespread in Central Africa, and epidemics had been reported within the 1920s and 1930s. The viral nature of the illness and the whitefly vector were demonstrated within the 1930s. Breeding efforts to develop resistant cassava had been profitable at first, but eventually the illness returned, and has continued to plague Central Africa. With the advent of molecular tools the viruses were characterized, and African cassava mosaic virus is just one of a group of associated viruses that trigger cassava mosaic illness. These viruses are within the household Geminiviridae, so named as a result of the particles are twin icosahedron. One drawback with management of African cassava mosaic virus is the abundance of the whitefly vector, which becomes more prevalent throughout epidemics. Another downside can happen when two completely different viruses infect the same plant, and a novel virus emerges that could presumably be a mixture of the genes of the 2 viruses. When we take a look at viral genomes we are ready to see that many viruses have developed this way, by recombining two different viruses to make a new virus. These new viruses could be more deadly than the unique viruses, and may sometimes bypass host resistance. The disease was first described in Fiji in 1889, although it was not known then that it was attributable to a virus. The virus is spread by movement of contaminated plant materials, and domestically by aphids. It spends its entire life within the phloem of the plant, the tubes contained in the plant that transfer sugars from photosynthesis and other vitamins between the higher and lower elements of the plant. This implies that to be transmitted the aphid vector has to probe into the phloem, and aphids do that only after they settle in for a long feed. Viruses that reside in the leaf cells could be acquired and transmitted by brief probing by the aphid. A full virus consists of six completely different particles, all looking similar by electron microscopy. It was answerable for "purple oat" epidemics in the late nineteenth and early twentieth centuries, the place oat vegetation turned pink in the field, and grain yields had been greatly reduced. In parts of the western United States, Barley yellow dwarf virus aids invasion by unique grasses that critically threaten native grasses. The unique grasses are heavily contaminated and likewise appeal to the aphid vectors, which then transmit the virus to native grasses which may be extra prone to the disease brought on by the virus. Barley yellow dwarf is a really well-studied virus that has an intimate relationship with its aphid vector. Specific strains of the virus are transmitted by different aphid species, and the aphids should feed on the plants, quite than just probing them, each to acquire and transmit the virus. In laboratory experiments aphids that had been carrying the virus most popular to feed on uninfected crops, while aphids without the virus most popular to feed on infected plants. The virus manipulates the manufacturing of plant compounds that appeal to aphids, to improve its spread. Recent research of plant genomes present that the ancestors of Cauliflower mosaic virus were integrated into plant genomes naturally more than 1,000,000 years ago. One of the latest discoveries about this virus is that it could sense when an aphid begins feeding on its plant host and rapidly creates a brand new type that the aphid can purchase. In the 1930s a severe citrus illness outbreak occurred in Brazil, and large numbers of timber died. The virus was referred to as tristeza, Portuguese for unhappiness, due to the devastation it triggered. In addition, contaminated vegetation within the subject typically have a quantity of strains of the virus on the similar time. Citrus tristeza virus may be transmitted by a quantity of aphid species, however the brown citrus aphid is the most efficient vector. This aphid was introduced into Florida, in the United States, from Cuba, within the Nineties and the spread of the virus elevated dramatically. The aphid can also be present in Asia, sub-Saharan Africa, New Zealand, Australia, the Pacific Islands, South America, and the Caribbean area. It is usually not discovered within the Mediterranean, and has not moved to areas of the United States exterior of Florida, although other aphid species can transmit the virus in these areas. The totally different lengths mirror the truth that these particles are fragile and a few are damaged during the purification and staining process. Later, when molecular instruments became available, it turned out that about 40 described plant viruses had been actually Cucumber mosaic virus. Cucumber mosaic virus has been documented in 1,200 different species of vegetation, making it the virus with the broadest identified host range. It infects many crop and backyard crops, and has triggered critical ailments around the world.
Nitroglycerin 2.5 mg generic on-lineTwo small vessels treatment upper respiratory infection 2.5 mg nitroglycerin order mastercard, which pass into the muscle fibers of the subscapularis treatment integrity nitroglycerin 6.5 mg mastercard, are coagulated. Numerous small nerves may be seen entering the muscle stomach of the subscapularis; vessels in the best way of subscapularis cut up are cauterized. Care must always be taken to level the electrocautery towards the subscapularis and away from the brachial plexus. The electrocautery (1 portal) is medial to the coracoid (on the inferior edge of the pectoralis minor). Dissection medial to the coracoid: the pectoralis minor tendon is recognized and incised with the assist of an electrocautery, all the time preserving contact with bone. The electrocautery is used as a blunt dissection probe and the delicate tissue medial to the coracoid is teased away. Followed by this, the posterior chord is visualized, which in flip guides the surgeon to the axillary artery. It must be famous that small punctate bleeding that happens is coagulated utilizing the electrocautery going through away from the plexus, thereby minimizing the chance of thermal harm to the nerves. Dissection under the coracoid: Visualizing through the D portal and alternating between the I and J portals, the lump of fat beneath the coracoid is excised using cautery. The cautery is switched from the I to the M portal for full visualization of the undersurface of the coracoid. These must be meticulously coagulated, as an excellent view of this area is crucial for completing a coracoid osteotomy. Dissection on the superior surface of the coracoid: the superior surface of the coracoid consists of the remnant of the acromioclavicular ligament and bursal tissue. A global view of the coracoid must be attained while trying in from the I portal. The first assistant controls the arthroscope and a second assistant flexes the arm in neutral rotation, allowing the surgeon to use both palms for finishing the steps. The best spot should be such that the tip of the information is roughly 5 mm posterior to the tip of the coracoid. It must be inserted via the skin in oscillation mode to stop damage to the cephalic vein. The information wire should be eliminated prior to advancing the cannulated drill to prevent damage to the plexus. The holes (9 mm apart) are then tapped utilizing the faucet provided and the top hats are inserted. Coracoid osteotomy: A 5-mm burr is introduced via the M portal whereas visualizing via the I portal, and the undersurface of the neck of the coracoid is burred to create a stress riser. A B by inserting the osteotome superiorly and finishing the managed osteotomy. A contemporary backflow of bleeding is attained and transient hyperpressure is attained utilizing the pump. Subscapularis split: the arm is adducted and held in neutral rotation with out traction, visualizing via the J portal and dealing by way of the I portal. This step is necessary for shielding the axillary nerve and safely finishing the subscapularis split. The superior border of the subscapularis is recognized adjacent to the rotator interval, and its inferior margin is identified by the anterior circumflex artery and its 2 veins (3 sisters). Creating inner and external rotation, the subscapularis split is made with the electrocautery always pointing away from the axillary nerve. A switching stick is inserted via the A portal traversing the joint and thru the subscapularis cut up. Care should be taken to maintain a lateral direction such that the tip of the switching stick is always lateral to the plexus. The coracoid osteotome is now inserted via the M portal and positioned over the glenoid neck by way of the break up and the second assistant now maximally externally rotates the arm to cause a blunt break up of the medial fibers of the subscapularis. Two switching sticks, one from the A portal and one from the J portal, are used to retract the superior and inferior fibers of the subscapularis. Back bleeding is encountered from the bone and small perforators entering the bone via the subscapularis muscle belly are cauterized. The coracoid plastic cannulated information is introduced through the M portal and the ultimate position of the graft is ascertained. The guide is inserted and a pair of information wires are drilled into the glenoid neck with the ideas of the wires exposed outside of the patient and held with artery forceps. These wires must be parallel to one another and the switching stick inserted by way of the A portal to ensure parallelism. The cannulated drill information is used to assist drilling both cortices and the anticipated length of screws famous. The cannulated trocar from the Latarjet set is threaded over the inferior guide wire from the posterior skin puncture and is advanced anteriorly till it appears on the anterior glenoid neck. The information wires are now removed from the posterior facet of the affected person, leaving behind the secured the cannulated trocar. Coracoid retrieval and ultimate preparation: the arm is flexed and the double cannula is introduced (with the deal with facing superiorly by way of the M portal). Visualizing from the I portal, the cannula and its 2 high hat screws are superior to be able to mobilize and switch the coracoid. The surgeon eburnates the undersurface of the coracoid utilizing a 5-mm burr via the J portal. Complete decortication of the undersurface of the coracoid is advisable to ensure union. It must be famous that the coracoid have to be held nonetheless to forestall inadvertent slips inflicting injury to the important neurovascular buildings. Coracoid fixation: the arm is internally rotated and the coracoid is inserted through the subscapularis cut up. The inferior hole (adjacent to the origin of the conjoined tendon) in the coracoid is guided over the cannulated trocar. The visualization is changed between the J and the D portal to ensure that the graft is well in touch with the glenoid. Any failure of conformity may be addressed by burring the sharp edges via the E portal. The shoulder is taken by way of abduction and exterior rotation and evaluated for stability and graft fixation. Postoperative Protocol Most sufferers are discharged the subsequent morning after their postoperative x-rays are checked. No physiotherapy is really helpful initially and sufferers are encouraged to actively elevate and move their arm. Complications encountered include the next: Hematoma postoperatively: Seen sometimes, sufferers usually complain of postoperative swelling of the hemithorax.
|
