Cheap 10 mg metoclopramide with visaWith the newer da Vinci S and Si robots gastritis diet ideas 10 mg metoclopramide discount with mastercard, this limitation on working length is no longer a big issue gastritis symptoms palpitations 10 mg metoclopramide cheap with visa. The digital camera is normally positioned above the umbilicus by way of a 12-mm port inserted utilizing a blunt-tipped trocar, although other descriptions have the port placed lateral to or beneath the umbilicus. A transverse curvilinear incision on the perimeter of the umbilical crease is employed as this provides for higher cosmesis on the pores and skin level and a stronger fascial closure. Recent evaluation of outcomes data from our establishment has demonstrated the physical Bovie Surgeon Console A 1122 Section 6 Laparoscopy and Robotic Surgery: Laparoscopy and Robotics in Adults toneal method [23�25], citing decreased risks of bowel injury and postoperative ileus as a number of the advantages [23, 26]. In addition, institutional variations exist as to whether or not to take an anterior approach [17, 27, 28] or a posterior method to the seminal vesicles, as described initially by the group from Montsouris [13]. Understanding that surgeon preference is most likely going probably the most important factor in determining which strategy is employed, we prefer a transperitoneal, anterior method with antegrade dissection. Using the precept of triangulation, dissection within the caudal course provides for better visualization of the buildings being dissected, as compared to making an attempt to see around the bulky prostate and dissecting back in direction of the bladder. It additionally allows the surgeon to perform the customarily difficult apical dissection after mobility of the prostate has been established. As for the right arm, whereas some prefer to use a monopolar hook or monopolar flat spatula, we favor a pair of monopolar scissors. Anterior bladder mobilization and retraction suture After profitable placement of all trocars and confirmation that each one devices are in working order, utilizing a 0� laparoscope, an inverted "U"-shaped incision is made in the anterior peritoneum from one inguinal ring to the other, with the bottom of the "U" placed close to the umbilicus throughout both medial umbilical ligaments. The arms of the "U"-shaped incision ought to be carried down to the inguinal ring until the crossing vas deferens is recognized, thus allowing for sufficient mobilization of this bladder-containing "flap. Care should be taken to not traumatize the pelvic bone as this can result in meddlesome bleeding that can usually be tough to management. Once the bladder is absolutely mobilized, we suggest a full-length 3-0 monocryl retraction suture be placed on the prime of the urachus and be introduced out through the 5-mm assistant port found in the best higher quadrant of the stomach. It additionally serves to shield both the massive and small bowel from inadvertent upstream thermal harm as the bladder "flap" separates all devices from the bowel (see Video ninety one. The fatty tissue overlying the prostate is removed so as to improve visualization of the puboprostatic ligaments, dorsal vein, and anterior bladder neck. Although not routinely carried out at all institutions, we consider that this maneuver facilitates the apical dissection and reduces the danger of anterior apical constructive margins. Furthermore, the lateral limits of this fatty tissue are in direct anatomic continuation with area three of an extended pelvic lymph node dissection. This ensures a safer staple line by compressing all edema and vascularity out of the tissues. However, we prefer the consistent and reproducible impact of stapling as it reliably offers a visual landmark to transect the urethra, hence reducing positive apical surgical margins (see Video 91. Bladder neck transection this is the most common a half of the procedure with which inexperienced surgeons wrestle. There are a quantity of causes for this, however most prominent we consider is the absence of obvious visual landmarks, the innate pure anatomic variability of the junction, and the want to "feel" the distinction between the prostate and the muscle of the bladder. After the camera is switched to the 30� down scope, we first establish the posterolateral contour of the prostate. Next it helps to see or "feel" the prostatovesical junction by compressing or pinching the bladder at its junction with the prostate. The prostate will result in minimal tour of tissue, while compression of the bladder wall shall be evidenced by an obvious mobility within the tissue. In and out traction on the Foley balloon also aids in identifying the anterior bladder neck. Using the rules of traction and counter-traction to help in defining the detrusor muscle fibers, electrocautery is used to divide the abundance of arteries and veins that traverse this region. Once the anterior bladder is opened down to the urethra in the midline, the Foley catheter is recognized and deflated. The catheter tip is delivered in to the surgical area and the robotic fourth arm grasps the Foley through its eyelet and pulls it anteriorly in the path of the abdominal wall. Counter-traction is offered by clamping the outer portion of the Foley catheter to the surgical drapes. The bladder neck is then dismembered from the prostate using a bladder necksparing approach; nonetheless, you will want to open the bladder neck adequately to visualize the trigone and help in defining the angle of transection of the posterior bladder neck. Sometimes the bladder attaches with a Control of dorsal venous complex and apical dissection After the endopelvic fascia is incised with cold scissors, the prostate is mobilized laterally down to the membranous urethra, sweeping the levator muscle fibers off the prostate with little to no cautery used. It is essential to notice that constructive apical margins occur due to transection too close to the apical prostate. This dissection is carried out to the extent of the prostatic apex, staying close to the posterior floor of the prostate. It is essential to carry this dissection far sufficient distally to utterly mobilize the rectum off the prostatic apex, and thereby cut back the chance of rectal injury during the apical dissection and transection of the urethra. Posterior counter-traction of the rectum offered by the surgical assistant facilitates this dissection. The posterior bladder neck can be divided directly, making an attempt to keep away from inadvertent entry in to the posterior prostate. It is our choice to method the bladder neck laterally, coming into the area between the posterior bladder wall and the seminal vesicles. The dissection begins laterally the place a few of the anterior vascular pedicle continues to be current. Again, the muscle is reduce cold, which permits the dissection to proceed behind the posterior bladder neck in to the house anterior to the vasa and seminal vesicles. As in open surgical procedure, the surgeon must all the time be mindful of dissecting in to the ureteral orifices proximally and the prostate gland distally. Release of the neurovascular bundles With the posterior dissection complete, the lateral prostatic vascular pedicles are nicely uncovered as pillar-like buildings. Authors have described using locking hemostatic clips [33] or bulldog clamps [34, 35]. This avoids the need to develop windows in the pedicle for placement of clips, which might usually result in bleeding, as properly as the need for an experienced assistant who can place and take away clamps accurately and effectively (see Video ninety one. At 9 months after surgical procedure, the cautery group was shown to have a potency rate of 14. Over time, the cautery group did reveal restoration of sexual function; nonetheless, the cautery-free group continued to "outperform" in long-term evaluation, with a potency rate of 92% (vs 63. By fully mobilizing the prostate, the antegrade, Posterior dissection As mentioned earlier, the Montsouris technique entails preliminary dissection via the pouch of Douglas to dissect the seminal vesicles off the rectum posteriorly and the bladder anteriorly. If this approach has been taken, the transection of the posterior bladder neck will lead instantly in to this beforehand dissected airplane. A theoretical disadvantage to this method is that every one sympathetic nerves coursing from the hypogastric autonomic plexus, between the lateral ideas of the seminal vesicles and the bladder neck, are divided. All testis cancer surgeons are aware of the complication of retrograde ejaculation due to an incompetent bladder neck, which happens when these nerves are resected. Initially, the proper or left vasa and seminal vesicles are identified and dissected totally as a unit fully all the way down to the tip of the seminal vesicle. With one vas deferens and seminal vesicle dissected, the robotic fourth arm or surgical assistant uses these buildings to present further anterior traction on the prostate. This facilitates a better dissection of the vas deferens and seminal vesicle on the contralateral aspect.
Metoclopramide 10 mg buy free shippingMetaanalysis of pores and skin adhesions versus sutures in closure of laparoscopic port-site wounds gastritis diet ����������� order metoclopramide 10 mg mastercard. For instance gastritis diet foods eat metoclopramide 10 mg order with visa, laparoscopic entry is often obtained by way of a wide range of initially blind punctures the place viscera and blood vessels are prone to unique accidents. Laparoscopy due to this fact requires a specialized information base, and demands a unique set of troubleshooting expertise. Whereas textbooks have been dedicated to laparoscopic problems, this chapter will cowl the primary areas pertinent to the urologist in coaching, in addition to for the working towards urologist wishing to broaden their knowledge. Since urologic laparoscopy is no longer in its infancy and surgical complexity has elevated, admonitions about problems from only a decade in the past might not be acceptable. For instance, open conversion is much less often required for the contemporary surgeon than it was prior to now (early sequence previous to 2000, conversion as high as 2. While the brink to convert must stay low, and the window to expeditiously tackle an evolving complication is short, the options and experience to intervene with out making an incision have expanded. The surgeon should train explicit care in the course of the studying curve; a number of research within the urologic [2, 3] and common surgical literature [4] have demonstrated an inverse relationship between surgeon experience and complication charges. Complications shall be organized by main category: (1) entry, (2) physiologic, (3) patient positioning, (4) end-organ (vascular, bowel, strong organ), (5) postoperative, and (6) miscellaneous. Where acceptable, issues pertaining to particular urologic procedures will be highlighted. Since robotic techniques have essentially duplicated laparoscopic counterparts for all procedures, all problems discussed herein and their management are generalizable to robotic surgery. Access problems Regardless of the method to gain initial deliberate entry in to the peritoneal (or retroperitoneal) cavity, entry remains a big supply of morbidity and potential mortality. The incidence of any kind of entry harm ranges from 5 in 10 000 to 3 in one thousand [6]. In a current literature evaluation of forty one articles, together with virtually 700 000 procedures for which Veress needle entry was used, 1575 (0. Upon transperitoneal entry, the blunt cannula springs back in to place, theoretically blunting the needle tip. This method may be employed alone in a desufflated abdomen or following initial insufflation by way of a closed (Veress) needle. A 2008 Cochrane literature evaluation evaluating open and closed entry methods found that there was insufficient proof to recommend one technique over one other [10]. Generalized under-reporting of complications additional hampers attempts to outline the true incidence of entry problems. Bowel damage is equally likely with open and closed entry methods [12], however there may be the next probability of quick analysis with an open method, for the rationale that injured bowel is directly visualized. Even so, delayed prognosis of bowel damage has occurred following open access as properly [13]. In our opinion, for instance, Veress needle security checks, such as aspiration and saline drop, can provide valuable clues when performed accurately and in conjunction with verifying a low opening stress (ideally < 9 mmHg). A revealed report on this matter, however, concluded that the ancillary needle checks provided little helpful info aside from opening strain [14]. The literature have to be interpreted with warning on this arena, since the most important think about gaining protected access is surgeon familiarity and mastery of a given strategy. When the surgeon encounters problem gaining entry by any strategy, the admonition to change something is prudent. A quote extensively attributed to Einstein captures this idea: "The height of insanity is repeating the same factor over and over and expecting Table one hundred and one. A potential reason for excessive opening stress (Veress access) aside from preperitoneal needle placement is incomplete affected person relaxation � After the trocar has been placed, look in with the digicam instantly. If vascular harm has occurred, the window for diagnosis and intervention is short. Do not waste treasured time cleaning the digital camera lens prior to your first look inside a different end result. In a difficult access scenario, careful reassessment of landmarks, checking for defective equipment, and evaluating approach angles, can make all the difference. Also, be aware that in overweight patients, dependable surface landmarks, such because the affiliation between the umbilicus and aortic bifurcation, are misplaced. Physiologic issues Pneumoperitoneum is associated with potential issues and physiologic alterations each from its mechanical compressive effects on blood vessels and viscera, and by its potential entry in to the bloodstream and subcutaneous tissues. An unfortunate by-product of its favorable diffusion properties is the potential to decrease blood pH with extended absorption. Patients with severe pulmonary disease in whom the ability to 1232 Section 6 Laparoscopy and Robotic Surgery: Exit Strategy and Complications stress insufflation immediately in to a serious vessel is the trigger. Subcutaneous emphysema is often clinically insignificant and resolves without particular intervention. Alternatively, a mix of a comfortable skin incision and loose fasciotomy round a trocar permits gradual improvement of ongoing subcutaneous emphysema during the period of a case. The presence of subcutaneous emphysema underscores the ability of pressurized gas to diffuse between body compartments [20]. While other pulmonary modifications are greatest considered expected alterations quite than problems, they warrant point out nonetheless. With mechanical ventilation, the scientific penalties are usually insignificant [16]. The mechanical compressive results of pneumoperitoneum on the diaphragm causes increased intrathoracic strain, increased peak airway stress, and decreased very important capability. Hemodynamic results of pneumoperitoneum are variable and troublesome to generalize [16], however a recent potential study by Meininger et al. Importantly, cardiac output was not affected both by Trendelenburg position or by pneumoperitoneum. The reader should note that other research have demonstrated conflicting outcomes in this enviornment. First, the patient is discovered to have profound bradycardia as an initial response to peritoneal insufflation. In this difficult situation, the surgeon must proceed quickly without putting the affected person at risk from overly aggressive trocar insertion. Attention to protected trocar placement is properly value a few additional seconds of bradycardia. Second, if an air embolus is suspected, the customarily cited Durant maneuver [18] is usually recommended to prevent the "air lock" from sitting in the best ventricular outflow tract. In the original examine, animals that were positioned left side down had improved hemodynamics. In this place with the best facet up, and moreover in Trendelenburg, theoretically the air is prevented from coming into the pulmonary outflow tract. Nevertheless, the presentation of air embolus is dramatic, especially if Veress needle excessive Complications of patient positioning the surgeon usually relies on gravity and affected person positioning for adequate exposure during minimally invasive genitourinary procedures. In a big sequence of urologic laparoscopic procedures compiled from 15 centers and over 1600 circumstances, the overall incidence of neuropraxia was 2. Risk factors included weight problems, longer operative occasions (>5 h), and superior patient age.
Diseases - Langer Giedion syndrome
- Kantaputra Gorlin syndrome
- Familial non-immune hyperthyroidism
- Immotile cilia syndrome, Kartagener type
- Arterial tortuosity
- Optic nerve coloboma with renal disease
10 mg metoclopramide order with amexClinically vital remnants could also be easily missed and left untreated underneath these circumstances [84 gastritis diet ����� 10 mg metoclopramide buy visa, 85] gastritis diet 7 day metoclopramide 10 mg cheap amex. It is associated with a shorter laser pulse length, wider fiber diameter, upper ureteral web site, and small stone measurement. Performing lithotripsy at low energy with little irrigation and actively extracting each fragment as quickly because it breaks from the stone might prevent stone migration [84]. Repositioning the stone to another calyx or pelvis, lower calyceal occlusion by autologous blood clot and flank place may also aid in retrograde calyceal stone therapy [90�93]. A recent research randomized, patients to active retrieval versus spontaneous passage of stones Chapter fifty eight Management of Residual Stone Fragments throughout holmium laser ureterolithotripsy [84]. In the latter group, the stone was completely turned in to dust or fragments of lower than 2 mm, which have been left in situ. There was no statistical difference in hospitalization, need for ache analgesia, time to full recovery, stone-free price, and wish for ancillary procedures at 30 days of follow-up. Moreover, because the period of follow-up will increase, the speed of complications and the necessity for intervention due to symptomatic episodes additionally increase. When left untreated, approximately half of these sufferers will experience a stone-related occasion, for which greater than half will require a secondary surgical intervention. Appropriate stone disintegration and removing of all stone fragments must be the purpose of every ureterolithotripsy. How significant are clinically insignificant residual fragments following lithotripsy. The fate of residual fragments after extracorporeal shock wave lithotripsy monotherapy of infection tones. Contemporary urological intervention for cystinuric patients: quick and long-term influence and implications. Clinical implications of clinically insignificant stone fragments after extracorporeal shockwave lithotripsy. Residual fragments after extracorporeal shockwave lithotripsy: Spontaneous clearance or risk issue for recurrent stone formation. Computed tomography versus intravenous urography in diagnosis of acute flank ache from urolithiasis: a randomized examine comparing imaging prices and radiation dose. Value of ultrasonography and helical 672 Section 5 Stone Management in Urology: General Principles computed tomography in the diagnosis of stone-free sufferers after extracorporeal shock wave lithotripsy. The accuracy of noncontrast helical computed tomography versus intravenous pyelography in the suspected acute urolithiasis: a meta-analysis. Renal stone detection using unenhanced multidetector row computerized tomography-does part width matter Two years follow-up of patients treated with extracorporeal shock wave lithotripsy. Does further extracorporeal lithotripsy promote clearance of small residual fragments Extracorporeal shock wave lithotripsy retreatment ("stirup") promotes discharge of persistent caliceal stone fragments after main extracorporeal shock wave lithotripsy. Mechanical percussion, inversion and diuresis for residual decrease pole fragments after shock wave lithotripsy: a potential, single blind, randomized managed trial. Randomized controlled research of mechanical percussion, diuresis, and inversion remedy to assist passage of lower pole renal calculi after shock wave lithotripsy. Effect of alkaline citrate therapy on clearance of residual renal stone fragments after extracorporeal shock wave lithotripsy in sterile calcium and an infection nephrolithiasis patients. Effect of potassium citrate therapy on stone recurrence and residual fragments after shockwave lithotripsy in lower caliceal calcium oxalate urolithiasis: a randomized managed trial. Effect of potassium citrate therapy on stone recurrence and regrowth after extracorporeal shockwave lithotripsy in kids. Is there a job for tamsulosin within the therapy of distal ureteral stones of seven mm or less Adjunctive medical therapy with an -1A-specific blocker after shock wave lithotripsy of lower ureteral stones. Nephrolithiasis scientific guidelines panel abstract report on the administration of staghorn calculi. Evaluation of fragmentation with single or multiple pulse setting of Lithoclast for renal calculi during percutaneous nephrolithotripsy and its influence on clearance. Chapter fifty eight Management of Residual Stone Fragments mizes stone migration during percutaneous nephrolithotomy. Residual stones after percutaneous nephrolithotomy; sensitivities of various imaging strategies in renal stone detection. Which is the most effective performing imaging methodology for demonstrating residual renal calculi Confident intraoperative choice making throughout percutaneous nephrolithotomy: does this affected person want a re-assessment Combination "sandwich" therapy for in depth renal calculi in 100 consecutive patients: immediate, long-term and stratified results from a 10-year expertise. Intraoperative fragment detection during percutaneous nephrolithotomy: analysis of excessive magnification rotational fluoroscopy mixed with aggressive nephroscopy. Prone retrograde laser lithotripsy facilitates endoscope-guided percutaneous renal access for staghorn 673 fifty three. Effect of medical administration on recurrent stone formation following percutaneous nephrolithotomy. Experience with percutaneous nephrostomy, extracorporeal shock wave lithotripsy and chemolysis in the remedy of obstructive uric acid stones. Randomized trial of stone fragment lively retrieval versus 674 Section 5 Stone Management in Urology: General Principles spontaneous passage throughout holmium laser lithotrpsy for ureteral stones. Outpatient holmium laser lithotripsy utilizing semirigid ureteroscope: Is the therapy outcome affected by stone load Assessment of novel ureteral occlusion system and comparability with Stone Cone in prevention of stone fragment migration during lithotripsy. How to avoid accumulation of stone fragments within the lower calyx throughout versatile uretero-renoscopy. Prospective, randomized trial evaluating shock wave lithotripsy and ureteroscopy for decrease pole caliceal calculi 1 cm or much less. Flank position ureterorenoscopy: new positional method to aid in retrograde caliceal stone treatment. The effect of ureteral stent placement on postureteroscopy complications: a meta-analysis. Ureteric stents compromise stone clearance after shockwave lithotripsy for ureteric stones: outcomes of a matched-pair evaluation. Efficiency and price of treating proximal ureteral stones: Shock wave lithotripsy versus ureteroscopy plus holmium: yttriumaluminum-garnet laser. Computed tomography-determined stonefree charges for ureteroscopy of upper-tract stones. Mandela School of Medicine, Greys Hospital, Pietermaritzburg, South Africa Introduction Acute renal colic might be probably the most painful event a person can endure. It is up to the attending doctor or urologist not solely to make the prompt prognosis but additionally to initiate efficient ache control and establish probably difficult renal colic. Classic presentation of renal colic: signs and indicators Patients with acute renal colic classically current with a sudden onset of severe ache originating in the flank. The pain usually waxes and wanes in severity, and develops in waves or paroxysms that are related to movement of the stone within the ureter and associated ureteral spasm. Pain is assumed to happen primarily from urinary obstruction with distention of the renal capsule.
Metoclopramide 10 mg order amexThey are designed with a high-frequency noise filter to stop malfunction from the vitality interference [106�108] gastritis diet zx buy generic metoclopramide 10 mg on-line. However gastritis diet indian buy metoclopramide 10 mg visa, electromagnetic interference is a vital explanation for pacemaker malfunction. In an emergency, a magnet can be placed over a standalone pacemaker to convert it to an asynchronous mode. However, Anesthesia for ureteroscopy With the appearance of smaller and semi-rigid versatile ureteroscopes, intravenous sedation is favorable for instances of brief length similar to cystoscopy and stent insertion. Ureteral stents, renal calculi, and ureteral strictures have been efficiently performed utilizing lidocaine 4% gel to anesthetize the urethra. This anesthetic method has the advantage of sooner working room turnover and sooner discharge from hospital [110�116]. Among men, discomfort throughout inflexible ureteroscopy appears to be associated to the passage of the instrument via the membranous Chapter 60 Anesthesia for the Endourologic Management of Stone Disease 697 urethra and bladder neck [110]. Pain appears to be better tolerated in girls having the process beneath native or intravenous sedation [95]. Due to the reality that the kidneys usually transfer with the respiratory cycle, the stone is just intermittently visualized [46, 47]. It is imperative that the anesthesiologist and urologist work together to permit concomitant adequate ventilation and intermittent apneic episodes to efficiently fragment stones. Urethral trauma with patient movement is a priority during ureteroscopy, emphasizing the importance of choosing an acceptable anesthetic method for a given patient. Selection of anesthetic agent may be tailored to the reality that most of these procedures are performed on an outpatient foundation and the patient will be going residence on the day of the procedure. The urethra receives innervation from the preganglionic sympathetic fibers of the T10�L2 spinal segments. The higher ureter receives parasympathetic enter from vagal fibers by means of the celiac plexus and the lower ureter from S2 to S4 [110]. Spinal and epidural anesthesia are not often the anesthetic selections for ureteroscopy as a end result of different modalities supply advantages over neuraxial strategies [110]. However, neuraxial anesthesia stays an option in patients with considerably poor respiratory reserve. It is an environment friendly method for ureteroscopy, cystoscopy, and stent placement in a majority of sufferers. Lesions at the degree of T6 and above are associated with a life-threatening, hypertensive emergency, during which uncontrolled sympathetic and parasympathetic hyperactivity happens in response to stimulation below the level of the spinal lesion [117�119]. This syndrome, known as autonomic dysreflexia, outcomes from the dearth of supraspinal control of the sympathetic neurons and altered neurotransmission within the spinal wire [119]. Stimuli such as bladder or bowel distention and ache throughout surgery can trigger extreme, uncontrolled hypertension and bradycardia. These sufferers will experience increases in pulse strain, sweating, piloerection, vasoconstriction under the level of the spinal lesion, and vasodilation above the spinal lesion. The issues resulting from autonomic dysreflexia embrace intracranial and retinal hemorrhages, myocardial infarction, coma, and demise. Cardiac rhythm anomalies corresponding to atrial fibrillation, ventricular tachycardia, and cardiac arrest can even happen [120]. General and spinal anesthesia blunt the afferent and efferent autonomic neural impulses. These two types of anesthesia are most well-liked over other strategies for sufferers with spinal wire damage. Autonomic dysreflexia could be treated with intravenous ganglion blockers, nitrates, clonidine, and calcium channel blockers. Oral nifedipine given 30 min before cystoscopy has been proven to alleviate the syndrome [121]. Bladder emptying and colonic decompression prior to a surgical process may help cut back the danger of growing autonomic dysreflexia. Despite the comparatively noninvasive nature of the procedure, there remains the potential for fast fluid shifts with the affected person within the prone place in addition to other potential mitigating components similar to hypothermia and potential bacteremia. Close monitoring and a focus are important in each the intra- and postoperative intervals, in addition to communication with the urologist to guarantee the best outcome for the patient. Subcutaneous bupivicain infiltration and postoperative pain perception after percutaneous nephrolithotomy. Instillation of pores and skin, nephrostomy tract, and renal puncture website with ropivicaine decreases pain and improves ventilatory perform after percutaneous nephrolithotomy. Haemodynamic results of the inclined position: a comparability of propofol whole intravenous and inhalation anaesthesia. Comparison of the results of sevoflurane and whole intravenous anesthesia in percutaneous nephrolithotomy. The pharmacokinetics of dexmedetomidine in volunteers with severe renal impairment. Visual loss as a complication of non-ophthalmic surgery: a evaluation of the literature. Head rotation, flexion, and extension alter endotracheal tube place in adults and children. Percutaneous endourologic procedures in high-risk sufferers within the lateral decubitus place underneath regional anesthesia. All of those issues can be handled safely as long the anesthesiologist and surgeon talk about all of those factors earlier than induction of anesthesia. Sleeprelated respiratory issues, loud snoring and extreme daytime sleepiness in obese topics. A Systemic Review of Obstructive Sleep Apnea and Its Implications for Anesthesiologists. Low-dose bupivicaine spinal anesthesia for percutaneous nephrolithotomy: the suitability and impace of adding intrathecal fentanyl. The results of irrigation fluid on core temperature in endoscopic urological surgery. Perioperative upkeep of normothermia reduces the incidences of morbid cardiac events: A randomized medical trial. Cuff-leak check for the analysis of higher airway obsturction in adults: a systematic evaluate and meta-analysis. Corticosteroids to stop extubation failure: a systemic evaluation and meta-analysis. Cardiac arrhythmia and conduction disturbances during sleep in four hundred patients with sleep apnea syndrome. Stone and pelvic urine tradition and sensitivity are better than bladder uring as predictors of urosepsis following percutaneous nephrolithotomy: A potential clinical study.
Purchase 10 mg metoclopramide mastercardIf not reducible gastritis symptoms treatment mayo clinic 10 mg metoclopramide buy amex, the sac must be incised in a circumferential trend simply at or contained in the neck of the sac gastritis diet ppt discount metoclopramide 10 mg. A Chapter ninety five Incisional, Parastomal and Inguinal Hernia Repairs 1169 wide incision might compromise later closure of the peritoneum. Dissection and tried elimination of the amputated sac are pointless and pose a danger of neurovascular injury. The retained sac may fill with fluid postoperatively (groin seroma or scrotal hydrocele), but the assortment normally resolves inside a couple of weeks without sequelae. These ought to be avoided if potential, since they might retract underneath the strain of the pneumoperitoneum and lead to hemorrhage during attempted ligation. The prosthetic materials (usually polypropylene) is now introduced in to the abdomen by way of one of many bigger ports. The mesh is inserted by rolling or folding it in order that it can be passed down the port with a fine-tipped curved dissector. Once in the peritoneal cavity, the mesh is unfurled and manipulated in to the preperitoneal space. A third instrument port can generally be useful since it might be frustratingly awkward at times to get the prosthesis in to the right place. Some surgeons incise the mesh on one aspect in order that it could slip across the spermatic twine. The 5-mm hernia stapler, or tacker, is inserted through the midline or contralateral port and used to fixate the anterior edge of the prosthesis first, avoiding the epigastric vessels. A bimanual approach using the nonoperating hand to palpate the top of the stapler by way of the stomach wall facilitates exact placement. Applied strain should not be too firm or tacks will penetrate too deeply, risking nerve entrapment. Another trick is to partially deploy the tack and use one finish to "hook" the mesh and then guide it in to place. The superolateral tacks are placed subsequent, extending from the upper corner of the prosthesis only as far down as the iliopubic tract. The final tack(s), positioned within the iliopubic tract itself, should not be positioned too deeply lest nerves become entrapped. Finally, tacks are positioned in the iliopubic tract operating between the inferior edge of the prosthesis and the internal inguinal ring. Although fixation of the mesh is usually included as an integral step in descriptions of laparoscopic inguinal herniorrhaphy, the need of this step is controversial. Many surgeons feel that fixation is crucial to reducing hernia recurrence by preventing the mesh from rolling up and uncovering the hernia defect. Mesh fixation, on the opposite hand, has been linked to an increased incidence of nerve harm and incurs the elevated value of the tacking gadget (or elevated costs related to longer operative times if fixation is accomplished by suturing). Recent retrospective studies as nicely as potential, randomized trials have reported no important differences in operative time, nerve entrapment, problems, or recurrences between fixed and unfixed mesh repairs [75�77]. The intra-abdominal strain is decreased to inspect for hemorrhage and reduce pressure on the peritoneum. The peritoneal incision and any defects created throughout reflection of the peritoneum or incision of the hernia sac are closed over the prosthesis either with the stapler or by suturing. The staples or sutures should be positioned sufficiently shut collectively to prohibit inside herniation by way of the peritoneotomy. The port sites are inspected for bleeding from the inner facet of the abdominal wall. Ports are eliminated one by one underneath vision at 5 mmHg intra-abdominal stress and the gas is then evacuated from the abdomen. The 5-mm skin incisions are closed with subcuticular absorbable sutures and/or sterile skin tape. The muscles are break up within the midline, and gentle finger dissection creates a tunnel down towards the pubis. Choices at this stage are to insert a Hasson-type cannula and to start insufflating with gas to open up the preperitoneal area, to dissect with a blunt probe positioned through an operating laparoscope, or to use a dilating balloon to steadily carry the peritoneum off the physique wall and broaden the preperitoneal house. This mechanical expansion breaks strands of connective tissue that always persist when gas alone is used and will stop full growth of the preperitoneal space, requiring tedious dissection to 1170 Section 6 Laparoscopy and Robotic Surgery: Laparoscopy and Robotics in Adults as described earlier. A vital wire lipoma must be resected to allow a greater match of the mesh around the spermatic twine. The similar admonitions as for stapling the prosthesis during the transperitoneal procedure apply right here. The pneumoproperitoneum is released after removal of the ports beneath direct vision at a pressure of 5 mmHg, and sites are closed as described earlier. The easiest and least costly dilating balloon is made on the operating table by tying the center finger of a giant sterile surgical glove over the end of a sixteen F pink rubber catheter or different out there sterile tubing. Slow inflation of the balloon with approximately 1 L of saline or gas from the insufflator will safely expand the house to adequate dimensions. Alternatively, a commercially prepared dilating balloon could be purchased from considered one of a number of producers. One benefit of a variety of the generally obtainable units, the power to look by way of and direct the balloon as it dilates, can be duplicated as well by the surgeon at the working table by tying the finger of the glove over a long 10-mm laparoscopic cannula as a substitute of a catheter. The balloon�cannula is inserted in to the tunnel beneath the rectus muscle tissue and the insufflator is connected. When the laparoscope is inserted in to the balloon� cannula and the gas insufflated, the pelvic structures can be visualized via the balloon (albeit not too clearly). A last possibility for creation of the preperitoneal house is to insert a Veress needle, Hasson-type cannula, or dilating balloon instantly in to the preperitoneal space either at the hernia website or, ideally, just above the symphysis pubis. If the bladder has been drained by a catheter, correctly prior to all extraperitoneal herniorrhaphies, the suprapubic web site is fairly secure for gaining access. Secondary ports are inserted beneath vision from a 10-mm laparoscope positioned via the primary port as in transperitoneal procedures. The secondary ports ought to be positioned decrease down on the belly wall compared with placement throughout transperitoneal procedures to keep away from violation of the peritoneum. Some authors have recommended putting all three ports in the midline: one on the umbilicus, one simply above the symphysis pubis, and the third halfway between the opposite two. If inadvertent entry in to the peritoneal cavity happens, the fuel could be allowed to escape continuously by inserting a Veress needle percutaneously in to the peritoneal cavity. This will allow profitable completion of the procedure in an extraperitoneal fashion if the peritoneotomy is small. Nonetheless, with continued insufflation and gentle manipulation of the peritoneum off the pelvic sidewall, the suitable landmarks can be ascertained. Once oriented, the surgeon cleans off the transversalis fascia analogs and addresses the hernia sac Postoperative care If only a laparoscopic herniorrhaphy has been carried out, sufferers are discharged residence from the restoration room except uncommon circumstances counsel the need for inpatient observation. An oral analgesic is prescribed routinely, though they typically are used for only some days, if at all. The affected person is encouraged to resume normal exercise the next day, except for heavy lifting, which is restricted for the primary week.
Purchase metoclopramide 10 mg mastercardEx vivo biopsies Several studies have evaluated the accuracy of the ex vivo (in bench) biopsy for the analysis of renal tumors [6 chronic gastritis shortness of breath metoclopramide 10 mg trusted, 20 lymphocytic gastritis symptoms treatment metoclopramide 10 mg buy fast delivery, 21, 30, 31, 41, 42, fifty four, 55]. The accuracy of surgical excision (nephrectomy or partial nephrectomy) biopsies taken under direct imaginative and prescient had been compared to the definitive pathologic diagnostic of the surgical specimen in one hundred pc of the cases. In many of the research pathologists evaluating the biopsy have been blinded to the definitive histopathologic outcomes. The price of nondiagnostic biopsies various from 2% to 20% with a trend to be greater than in the trendy percutaneous biopsy studies [22]. This fact may be defined by the lack of visualization of the complete tumor, as can occur during imaging or within the absence of needle stabilization during percutaneous puncture. When interpreting the outcomes of in-bench biopsy studies, it has to be taken in to account that this ex vivo setting is only partially comparable to scientific follow, the place percutaneous biopsies would be the normal. A fee of biopsy failure as high as 37% has been reported in renal plenty smaller than three cm versus 9% in tumors bigger than 3 cm [52]. The rate of nondiagnostic biopsies is also Percutaneous biopsy in contrast with 100 percent surgical specimens the number of research on the accuracy of percutaneous renal mass biopsy based mostly on 100 percent comparability of the Chapter 110 Renal Mass Biopsy 1335 Table a hundred and ten. Fuhrman nuclear grade was appropriate in 68%, with a lower concordance than for subtype (60�100%), as was the case in larger renal lots [62�64]. The price of nondiagnostic biopsy varies from 0% to 23% in these collection of percutaneous ablation [71�74] and from 0% to 30% when tumor biopsy is carried out throughout laparoscopic ablation [75�80]. At least throughout laparoscopy-assisted ablation, modification of the biopsy technique, by activating the firing mechanism of the biopsy gun externally to the target tissue, led to a higher diagnostic yield in a small scientific collection [77]. The standards classifying a biopsy as nondiagnostic or benign varies between groups, which can explain the broad vary of nondiagnostic or benign results. As an example, normal renal tissue, fibrotic tissue or necrotic tissue are distinctly classed as benign by some and nondiagnostic by others [78, 80]. In reality, the stricter the nondiagnostic standards are, the upper the nondiagnostic fee of the biopsy. Tumor biopsies may also be taken immediately after ablation to decrease threat of bleeding or tract seeding. Success after ablation therapy is mainly decided utilizing cross-sectional imaging with contrast. Therefore, some facilities have carried out a further postablation biopsy to assess the success of the ablation. The 6-months postcryoablation biopsy was consistently adverse in all nonenhancing masses. The outcomes for cryoablation have been superior, with a sensitivity and specificity of 77. However, within the trendy series an general accuracy of 94% in figuring out the proper histologic subtype was reported [22]. This problem stays a challenge for the pathologist, especially when limited tissue is on the market, as is the case with biopsies. In all the discordant circumstances, the actual grade found in postoperative pathology was inside one grade of the grade discovered at biopsy. This information has not solely diagnostic purposes but may influence follow-up coverage. An additional use of biopsies within the frame of ablation therapy is in figuring out the presence of residual tumor. The formed antigen�antibody complicated may be visualized by (fluorescent) staining and due to this fact the presence of the antigen can be demonstrated. It is probably going that in the near future these techniques will contribute extra to the diagnostic course of [94�96]. As described earlier, this ends in the interobserver and intraobserver variability of subtyping [19, 20]. For a very long time research to improve subtyping of renal tumors had no priority since there have been no medical penalties. These attribute variations imply that the different subtypes are distinguishable by mapping this genetic expression. Conclusions and recommendations There is an growing curiosity and pattern to incorporate the percutaneous biopsy of a renal mass in to the diagnostic algorithm of small renal tumors, when therapy is dependent upon histologic subtype determination, and for ablative procedures. Modern series on percutaneous biopsy of renal masses show a high accuracy and a decrease fee of failed or undetermined biopsies than older collection. Although still scarce, these latest sequence with pathologic affirmation by the use of surgical specimen support these encouraging results. Biopsy immediately performed after ablation leads to the same diagnostic yield as before ablation as architectural construction remains to be recognizable. Nephronsparing surgery and percutaneous biopsies in renal-cell carcinoma: a global impression among endourologists. Prospective analysis of computerized tomography and needle biopsy with everlasting sectioning to decide the nature of strong renal masses in adults. Changes in the stage and surgical administration of renal tumours throughout 1995�2005: an analysis of the Dutch national histopathology registry. The evolving presentation of renal carcinoma in the United States: developments from the Surveillance, Epidemiology, and End Results program. A decade of surgically removed small renal plenty within the Netherlands: developments in pathological reporting and kind of surgery. Cytological punctures in the prognosis of renal tumours: a research on accuracy and reproducibility. Prospective evaluation of intraoperative frozen needle biopsy of stable renal plenty in adults. Effectiveness and safety of image-directed biopsies: coaxial technique versus typical fine-needle aspiration. Fine needle aspiration using improved agar microbiopsy is highly concordant with renal mass last prognosis and subclassification. Diagnosis of renal tumors on needle biopsy specimens by histological and molecular evaluation. Renal cell carcinoma sub-typing by histopathology and fluorescence in situ hybridization on a needle-biopsy specimen. Fine-needle aspiration of renal masses in adults: evaluation of outcomes and diagnostic issues in 108 instances. Ultrasound, angiography and nice needle aspiration biopsy in analysis of renal neoplasms. Diagnostic accuracy of computed tomography-guided percutaneous biopsy of renal masses. A preoperative prognostic nomogram for strong enhancing renal tumors 7 cm or less amenable to partial nephrectomy. The worth of preoperative needle core biopsy for diagnosing benign lesions among small, incidentally detected renal lots. Incidental renal tumours: the frequency of benign lesions and the function of preoperative core biopsy. Microsatellite allelotyping differentiates chromophobe renal cell carcinomas from renal oncocytomas and identifies new genetic changes. Effect of needle gauge, level of anticoagulation, and target organ on bleeding related to aspiration biopsy.
Chive. Metoclopramide. - Are there safety concerns?
- How does Chive work?
- Removing parasitic worms.
- What is Chive?
- Dosing considerations for Chive.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96415
Cheap metoclopramide 10 mg on-lineNow in the era of robot-assisted laparoscopic surgery gastritis diagnosis code purchase metoclopramide 10 mg without a prescription, urologic surgeons are incorporating this method for nephrectomy and nephroureterectomy gastritis znacenje cheap metoclopramide 10 mg without a prescription. This chapter will review the indications, techniques, and results for laparoscopic and robotic radical nephrectomy and nephroureterectomy. Whenever possible, T1a renal plenty are eliminated by way of using a partial nephrectomy [5]. If not amenable to minimally invasive techniques, then an open partial nephrectomy should be thought of. These embrace significant coagulopathy or comorbidities that preclude the affected person from present process common anesthesia. Reports have been published relating to the minimally invasive management of a renal vein thrombus, however this is restricted to highly experienced facilities [10]. Previous stomach surgical procedure has not demonstrated an elevated danger of either problems or want for conversion. This includes a detailed history and physical examination, an entire blood depend, serum electrolytes, coagulation panel, calcium, and alkaline phosphatase. A bone scan is unnecessary in the absence of bone pain or an elevated alkaline phosphatase. Abdominal imaging might help in hilar dissection by preoperatively figuring out a number of renal arteries or adherent anatomy. Finally, though lymphadenectomy for renal cell carcinoma remains controversial, cautious attention ought to be paid on imaging to regional and retroperitoneal lymphadenopathy. Some choose to use a bowel preparation so as to decompress the colon and small bowel for improved visualization and working area inside the abdomen. A single dose of an antibiotic agent is given 30 min prior to the first incision to cowl skin flora. Sequential compression gadgets are placed on the calves of the affected person and initiated previous to the induction of basic anesthesia, together with an optionally available dose of subcutaneous heparin. The affected person is then fastidiously placed in a modified lateral decubitus position, angled at roughly 30o from the bottom. Both legs are stored straight with a pillow or different padding positioned behind the knees for support. Finally, the stomach is prepped sterilely, together with the corresponding flank in case of a need to convert to an open procedure. Access the stomach is insufflated to a strain of 15�20 mmHg using a Veress needle. Once sufficiently insufflated, a 12-mm dilating trocar is positioned with using a 0o lens to guide its place in to the abdomen at the level of the umbilicus. The 0o lens is exchanged for a 30o 10-mm laparoscopic lens, and the abdominal contents are inspected for any damage from either the Veress needle or the first trocar. This could also be helpful within the case of previous stomach surgical procedures, although the utilization of Veress needle access is documented to be secure in this affected person group as well [15]. A second 12-mm trocar is positioned at the degree of the umbilicus in the anterior clavicular line. A third, 5-mm trocar is positioned approximately eight cm cephalad to the umbilical trocar in the midline. For a proper nephrectomy, an extra 5-mm port could additionally be placed inferior to the subxiphoid process in order to help with liver retraction. Furthermore, for significantly large renal plenty, all 12-mm ports must be used to enable for max versatility in passing a larger number of devices via any port location. Finally, if a further port is required for retraction, an ideal placement is within the previously marked Pfannenstiel incision line. At the completion of the case, the extra port incision is extended and used to extract the specimen. Laparoscopic transperitoneal nephrectomy Patient positioning the patient is initially placed in the supine position upon arrival within the working room. A airplane is developed between the posterior mesenteric and anterior perirenal fats utilizing a combination of blunt and sharp dissection. The respective colon is mobilized medially from the iliac vessels to the respective hepatic or splenic flexure. For a proper nephrectomy, the hepatic flexure is launched by dividing the renocolic ligament. Minimal use of blunt dissection is inspired across the duodenum to keep away from inadvertent serosal injuries. The left colon, in the case of a left nephrectomy, is mobilized equally with a mixture of blunt and sharp dissection. The splenorenal ligament and splenophrenic attachments are divided to have the ability to mobilize the spleen medially, en bloc with the splenic flexure, which offers medial reflection of the tail of the pancreas. This maneuver is essential to decrease the risk of injury to the tail of the pancreas throughout left hilar dissection. Complete splenic mobilization typically requires visualizing the stomach above the spleen. Alternatively, the mid ureter could be discovered posterior and medial to the gonadal vein. This relationship is especially necessary when tracing the ureter to the renal hilum in the case of a right nephrectomy. Care is taken to sweep the gonadal vein medially, separating it from the ureter and avoiding the chance for avulsing it from the vena cava. The ureter is stored intact, which allows it to be used as a handle for anterior and cephalad retraction of the kidney later within the case. This has the potential for causing important bleeding in the case of large, decrease pole masses or if a quantity of parasitic vessels are encountered. Prior to the beginning of dissection, we recommend putting a small lap pad in to the affected person. In the occasion of surprising bleeding, this can be utilized to enhance visualization, or within the worst case, tamponade bleeding to permit time for open conversion. With the lower pole of the kidney mobilized, the ureter may be traced cephalad to the renal hilum. Care must be taken when dissecting towards the renal hilum in the occasion of a lower pole accessory vessel. Retracting anteriorly and cephalad on the kidney permits for higher exposure to the renal vein and artery. Judicious use of energy-based dissection could additionally be required to divide the fibrous lymphatic tissue typically surrounding the renal artery. Next, when the left renal vein is isolated, the gonadal vein could be clipped and divided if necessary. Caution must be exercised at this point to stop avulsing a possible lumbar vein that may feed in to the posterior floor of the left renal vein. If the adrenal gland is to be taken, the left adrenal vein can be clipped and divided at this level.
Generic 10 mg metoclopramide visaReduction of cannula-related problems using a radially increasing entry system gastritis diet 90 safe metoclopramide 10 mg. The function of computerized tomography within the evaluation of complication after laparoscopic urological surgical procedure gastritis diet ketogenic metoclopramide 10 mg without a prescription. Randomized trial evaluating a radial expandable needle system with chopping trocars. Comparison of laparoscopic and open retropubic urethropexy for treatment of stress urinary incontinence. Laparoscopic orchiopexy for the palpable true undescended testicle: Preliminary expertise. Access and trocar placement is of critical importance as improper placement might lead to issue later. In this chapter we outline the required steps for proper affected person place, entry, and secondary trocar placement for both renal retroperitoneal surgery and pelvic extraperitoneal surgical procedure. In addition, we define potential exclusion standards for retroperitoneal renal/adrenal surgical procedure and extraperitoneal pelvic surgery. Finally, we briefly summarize critical points related to laparoscopic exit at the end of the case. No definitive exclusion criteria exist for retroperitoneal entry, although a couple of cases may present more challenges for retroperitoneal surgery. Renal tumors larger than 10 cm in dimension are best approached by way of a transperitoneal strategy. Those located on the posterior hilar aspect could present challenges with retraction and lifting of the kidney and as such may be better fitted to the transperitoneal method. Prior percutaneous entry for stone surgery has not introduced a significant challenge in our experience. Retroperitoneal renal/adrenal surgical access Direct access to the retroperitoneum for renal or adrenal surgery might supply several potential advantages over the transperitoneal method. Ligation of the renal artery and vein throughout radical nephrectomy could also be aided by circumventing the necessity for bowel dissection. In addition, in cases of posterior small renal masses, direct access to the posterior facet of the kidney might obviate the need for full renal mobilization. Patients with a number of prior transabdominal surgical procedures or massive anteriorly situated mesh may also benefit from the retroperitoneal strategy for renal or adrenal surgery. Patient position and entry method After induction of common anesthesia, the affected person is positioned within the full flank position. The patient is secured to the desk with 3-inch tape on the level of the chest (without impeding mechanical ventilation) and hips. Securing the affected person in this method permits the desk to be rotated from right to left. Pillows are positioned between the legs and pressure factors (knees, hips) are properly padded. The tip of the 12th rib is marked with semi-permanent ink prior to sterile prep and drape, as palpation of the rib after preparation and gloving may be impaired, especially in the overweight patient. At the intersection of this line and the decrease facet of the 12th rib, the left trocar is inserted. S-retractors are used to break up the exterior indirect muscle and often the internal indirect muscle tissue all the method down to the lumbodorsal fascia. At this point a 30� lens, 10-mm laparoscope is inserted through the dissecting balloon port and the anatomy is appreciated. The psoas muscle can typically be assessed posteriorly and the peritoneum anteriorly. The balloon dissecting trocar is deflated and a balloon working trocar (Covidien) is placed. Placement of secondary trocars Under direct imaginative and prescient the 2 remaining trocars are placed. This trocar may be angled in a barely extra cephalad direction, which will lower the quantity of torque on the trocar and surgeon fatigue in the course of the case. The peritoneum may be visualized and, if necessary, may be dissected more medially utilizing the surgical left trocar and a laparoscopic Kitner instrument. Access for extraperitoneal pelvic surgical procedure the application of pelvic extraperitoneal surgery is finest for robot-assisted laparoscopic prostatectomy. Other urologic applications embody distal ureter surgery, partial cystectomy of anterior lesion, and restricted pelvic lymph node dissection. An advantage of the method is decreased need for a steep Trendelenburg position during the procedure. Patients with multiple prior stomach surgeries (but virginal extraperitoneal space) with known or suspected bowel adhesions could additionally be ideal candidates. In the event of vesicourinary anastomotic leak, the leak is contained in the extraperitoneal area. Disadvantages embody the smaller working space and the upper fee of pelvic lymphocele if bilateral lymph node dissection is carried out. Patient exclusion the transperitoneal strategy is greatest for patients with prior extraperitoneal surgical procedure, corresponding to open simple prostatectomy, open bladder stone elimination, and renal transplantation. In such circumstances, it may not be possible to dissect the space of Retzius with the balloon for protected placement of lateral trocars. Patient position and entry method the affected person is placed in the supine place. Lower extremities could additionally be placed in Yellofin leg holders or using a split-leg table. An orogastric tube is positioned by anesthesiology, and the patient is ready and draped sterilely. S-retractors are used for retraction and dissection is sustained to the external fascia. Stay sutures of 0-vicryl are placed within the exterior fascia, caudal and cephalad to the incision web site on the fascia. A very skinny layer of investing fascia of the muscle (no correct posterior sheath exists at this level) is recognized and incised with scissors or blunt index finger dissection. Under direct vision with a 10-mm laparoscope, insufflation is sustained till the pubic bone is visualized from throughout the balloon. Care is taken to keep away from distraction of the inferior epigastric vessels during insufflation. Placement of secondary trocars It is necessary to push the peritoneum in a cephalad and lateral path to allow placement of lateral secondary trocars. Despite the use of the kidney-shaped dissecting balloon, we find it necessary to use a 10-mm laparoscope and some mild abdominal stress to sweep the peritoneum in a cephalad and lateral direction. Chapter 75 Retroperitoneal Access 877 Laparoscopic exit Although nice emphasis is placed on preliminary entry, of equal significance is the exit or removal of trocars at the end of the case. Here we describe the essential features of exit from retroperitoneal and extraperitoneal surgical procedure.
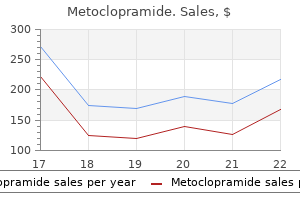
Purchase metoclopramide 10 mg otcSize (cm) * 6 Follow-up (months) * 26 Overall survival (%) 50 Disease-free survival (%) 50 Study Moinzadeh et al gastritis diet 5 2 order metoclopramide 10 mg. Patients with relative or absolute contraindications to laparoscopic surgical procedure must be thought of for an open surgical process gastritis sintomas 10 mg metoclopramide. Larger lesions are also technically difficult, partly as a result of they could distort the encircling anatomy. This can result in misinterpretation of the anatomic landmarks and increase the propensity in the path of critical, life-threatening complications. Patients present process adrenalectomy for large plenty should also be recommended on the potential of concurrent en bloc nephrectomy. Different types of endocrinologic problems can result in disease-specific problems. Patients with Conn syndrome are more doubtless to develop electrolyte abnormalities and require monitoring of blood pressure. In sufferers with pheochromocytoma, close perioperative monitoring of blood stress is essential. To avoid problems, care should be taken during creation of the pneumoperitoneum. The Veress needle must be placed in proper place to avoid damage to the liver, spleen, and intestines. During dissection, caution must be exercised to avoid damage to the encircling constructions such as the bowel and pancreas. When indicated, both a laparoscopic repair or open laparotomy ought to be carried out. Vascular problems are the most serious and will contain harm to the adrenal vessels, renal arteries and veins, and the inferior vena cava. Laparoscopic control of a vascular harm could additionally be tried with electrocautery or clips. In the postoperative interval, early ambulation is inspired to reduce the risk of a deep vein thrombosis. Chapter eighty five Laparoscopic and Robotic Adrenalectomy 1033 In selected patients, chest physiotherapy is required to forestall lung atelectasis. Postoperative shoulder pain is a common, although often a self-limited, complication. Bipolar coagulation could also be achieved utilizing standard electrocoagulators or modern energy-based devices, such because the LigaSure vessel-sealing system (Valleylab) or the ultrasonic coagulator (Harmonic scalpel). Bipolar coagulators can additionally be used for dissection, leading to much less trade of devices. They additionally take away the requirement for particular person dissection and isolation of blood vessels, minimizing avulsion and bleeding. However, the use of these instruments is limited by blood-vessel caliber and bigger veins will not be adequately controlled by these devices alone. Needlescopic instruments are outlined as those with a diameter of not extra than three mm, therefore leading to smaller incision than standard 5�12-mm ports. Besides higher cosmesis, needlescopic surgery might provide the benefit of reduced postoperative pain, hospital stay, and recovery time. It is important to notice that needlescopic adrenalectomy ought to solely be approached by skilled laparoscopic surgeons in rigorously selected patients [32]. This strategy preserves a higher hormonal reserve and should keep away from the need for hormonal supplementation following adrenalectomy. These devices permit for a minimal bleeding throughout transection of the adrenal parenchyma. Adrenalectomy is performed based on the steps of standard transperitoneal adrenalectomy using articulated or bent instruments that permit triangulation intracorporeally regardless of the close proximity of several instruments (dissector, grasper, and scissors) by way of a single port. These devices include roticulators (Covidien, 1034 Section 6 Laparoscopy and Robotic Surgery: Laparoscopy and Robotics in Adults intensive laparoscopic expertise. These progressive techniques require longer follow-up and extra information to assess their oncologic efficacy and perioperative outcomes. Therefore, they need to be approached with warning and only be attempted if the surgeon is confident of adhering to the ideas of oncologic surgery. We are currently witnessing a transition from conventional open to less and fewer invasive surgical approaches. The paradigm of open surgery for cancer is being continuously challenged and presently, with maturing laparoscopic experience, open procedures for adrenal lesions are being changed by minimally invasive approaches with comparable efficacy. Hemostatic agents (glues, Surgicel; Ethicon Endo-Surgery Inc) can be utilized for hemostasis when essential. Ablative methods (radiofrequency/cryo/chemical) Ablative techniques characterize the new frontier of minimally invasive approaches and supply the advantages of low invasiveness and fewer technical challenges in comparability with standard surgical procedure. These advantages could translate in to lowered morbidity because the process may be performed on an outpatient foundation. Ablation of adrenal neoplasms carries a significant threat of releasing a large amount of hormones quickly in to the bloodstream. Release of catecholamines can induce arrythmia or hypertension; thus, pretreatment with alpha- and beta-blockade is warranted. Chemical ablation has seen relative success within the management of encapsulated hepatic tumors and has now been utilized to adrenal neoplasm. The role of ablation in the remedy of adrenal tumors has but to be decided and there have been suggestions that its best potential lies in the therapy of recurrent illness, small biochemically lively tumors [42], as nicely as palliative care [43]. Ablative strategies are becoming more and more popular in the urologic subject with intensive fundamental and medical analysis endeavors in place. Technologic advances in imaging and precise targeting of the lesions will likely enhance the enchantment of these progressive approaches. However, till solid consequence data are mature, these techniques should be thought-about as experimental. Is laparoscopic adrenalectomy feasible for adrenocortical carcinoma or metastasis Laparoscopic renal and adrenal surgical procedure in overweight patients: comparability to open surgical procedure. This is an advanced laparoscopic process and must be undertaken only by these with Chapter eighty five Laparoscopic and Robotic Adrenalectomy 1035 14. A posterior lumbar approach for retroperitoneoscopic adrenalectomy: assessment of surgical efficacy. Comparison of laparoscopic transabdominal lateral versus posterior retroperitoneal adrenalectomy. Outcomes from 3144 adrenalectomies in the United States: which matters more, surgeon volume or specialty Laparoscopic adrenalectomy is superior to an open approach to treat primary hyperaldosteronism. Laparoscopic vs open adrenalectomy for the treatment of primary hyperaldosteronism.
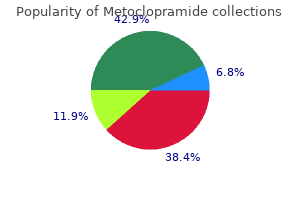
10 mg metoclopramide amexIt has widespread applications in human radiology gastritis nausea cure 10 mg metoclopramide generic otc, including prostate most cancers imaging gastritis symptoms treatment discount 10 mg metoclopramide mastercard. Endorectal coils are used both alone or together with phased-array floor coils. Targeting biopsies provides the advantage of detecting prostate most cancers which may not have been detected by systematic sampling alone, particularly those outdoors the peripheral zone [21, 22, 25, 26]. Although the outcomes of this method are encouraging, it also has certain limitations. Food and fluids are restricted from midnight the night before till after the procedure is complete. Before the process, per rectum examination is carried out to assess the area for safe probe insertion. The endorectal coil or balloon coil has a flexible shaft with a small balloon at one finish. Once inserted, the balloon is crammed with air till it is out there in to contact with and conforms to the size and shape of the prostate. A noninvasive imaging modality would represent a major breakthrough in prostate cancer diagnostics. On T1-weighted photographs, the prostate demonstrates homogenous medium sign depth. Furthermore, the accuracy of cancer detection also varies based on the dimensions of the tumor, location of the tumor, and biopsyassociated adjustments, which can cause incorrect estimation of tumor presence and extent. It is notoriously troublesome to distinguish biopsy-associated hemorrhage from tumors on T2-weighted photographs. However, these small foci may represent potential for clinical significance with growing time. The downside is that the dimensions of the tumor has not been proven to correlate well with want for therapy and thus, the rationale for energetic surveillance remains to be proven. Prostate tumor burden It is commonly found that pathologic staging, surgical margin status, histologic grade, and tumor quantity are highly effective predictors of particular person prognosis and prostate cancer biology [40�42]. Tumor volume estimated from prostatectomy specimens correlates with the chance of failure after radical prostatectomy [43], and tumor volumes lower than 0. Tumor volume measurement could due to this fact provide necessary info for therapy planning. An overestimation was seen in 47% of circumstances and an underestimation in 23% of cases [45]. The aim of imaging technology is to differentiate between ailments confined to the gland (T1�T2) and domestically invasive illness (T3). Patients with organ-confined illness could be handled with radical prostatectomy or radiation remedy, whereas these with more advanced disease are handled with radiation therapy, hormonal therapy or a mixture of these [49, 50]. As a end result, there was a significant increase in the capability to correctly define tumor location and extent, enhancing the ability to tailor the therapy choice to guarantee complete eradication of cancer while minimizing treatment-related morbidity. On the opposite hand, any bulging or irregularity within the contour of the gland, hypointense focal thickening of the capsule on the capsular margin or at the edges of the tumor, and retraction of the capsule adjacent to the tumor are highly suspicious indicators for capsular penetration [56]. Precise analysis of all of those options is crucial for correct remedy planning. This permits for a chance to preoperatively alter the surgical approach to enhance most cancers management, whereas preserving periprostatic tissue necessary for recovery of urinary and sexual perform. Although further trials will be necessary to outline the safety and oncologic efficacy of this outpatient procedure, its refinement could end in a reasonable, minimally invasive various to present active therapies. Intraprostatic tumor development is associated with elevated cell membrane turnover and elevated cell proliferation, which finally ends up in an increase in mobile choline and a lower in citrate ranges [90]. The temporal resolution of the dynamic acquisition for prostate imaging varies widely from 1�2 s up to 95 s, being largely within the vary of 2�20 s/ dynamic phase. Cancers can show a large, early enhancement adopted by a quick washout time�intensity curve. During the cancerous process, not only is there angiogenesis, however the construction and orderly organization of these blood vessel networks are also disrupted. The newly formed blood vessels have leaky endothelia and disrupted obstacles, which end in elevated permeability of vessels and extravasation of the contrast. This know-how can also be useful for detecting recurrent most cancers, as nicely as guiding targeted radiation therapy. Further studies are needed earlier than this promising technology enters within the clinical arena. Cancerous prostate tissue has an elevated cellularity, which lowers the obvious diffusion coefficient in comparison with the traditional prostate tissue, both within the peripheral zone [102] and within the transition zone [103], in flip causing a reduction in the move or diffusion of water [102, 103]. Early research with this technology report a high sensitivity (94%) and specificity (91%) within the peripheral zone, and a equally excessive sensitivity (90%) and specificity (84%) within the transition zone [108]. These nanoparticles are injected intravenously and are taken up by macrophages in normal lymph nodes. This creates a contrast between benign nodes and cancerous nodes where the macrophages have been replaced by tumor cells [109]. It has confirmed to be effective in a quantity of different cancers [109] and investigations in to its potential use in prostate cancer are ongoing. This will require the combined skills of scientists and physicians in the fields of molecular biology, pharmaceutical chemistry, radiology, pathology, and urology. The frequency of carcinoma and intraepithelial neoplasia of the prostate in young male patients. Predicted prostate specific antigen outcomes using transrectal ultrasound gland quantity. Endorectal magnetic resonance imaging as a predictor of biochemical end result after radical prostatectomy in men with clinically localized prostate cancer. Value of magnetic resonance spectroscopy imaging and dynamic contrast-enhanced imaging for detecting prostate most cancers foci in men with prior unfavorable biopsy. Prospective evaluation of prostate cancer detected on biopsies 1, 2, 3 and four: when ought to we cease Comparison of endorectal magnetic resonance imaging, guided prostate biopsy and digital rectal examination in the preoperative anatomical localization of prostate most cancers. Prevalence and characteristics of screen-detected prostate carcinomas at low prostate-specific antigen levels: aggressive or insignificant Morphologic and clinical significance of multifocal prostate cancers in radical prostatectomy specimens. The utility of magnetic resonance imaging and spectroscopy for predicting insignificant prostate cancer: an initial evaluation. Sextant localization of prostate cancer: comparability of sextant biopsy, magnetic resonance imaging and magnetic resonance spectroscopic imaging with step part histology. Stratification of pathologic options in radical prostatectomy specimens which may be predictive of elevated initial postoperative serum prostate-specific antigen ranges. Apparent diffusion coefficient of the prostate in males previous to biopsy: willpower of a cut-off worth to predict malignancy of the peripheral zone. Transurethral biopsy of the prostate for persistently elevated or growing prostate particular antigen following a quantity of adverse transrectal biopsies. Prospective analysis of endorectal magnetic resonance imaging to detect tumor foci in males with prior negative prostastic biopsy: a pilot study. Correlation of pathologic findings with development after radical retropubic prostatectomy. Estimation of prostate cancer quantity by multiple core biopsies earlier than radical prostatectomy.
|