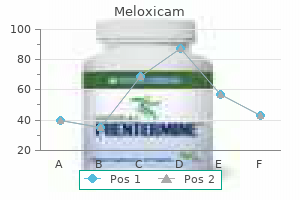
Meloxicam 15 mg order without a prescriptionC: Parasternal long-axis view confirms discordant ventriculoarterial connection: the pulmonary trunk by its abrupt posterior turn shortly distal to the pulmonary valve reactive arthritis in neck meloxicam 15 mg buy on-line, and (in other planes of this echo view) the aorta by the origin of the brachiocephalic artery arthritis treatment center purchase meloxicam 15 mg visa. The proper coronary artery, in one other echo aircraft, arises from the posterior proper aortic sinus. E,F: Echocardiographic pictures obtained at postoperative examination 1 year after surgical procedure (arterial change at thirteen days of age) exhibits reasonable dilation of the neoaortic) root. Catheterization findings are in preserving with the detailed discussions beneath the section on Physiology and with the classification schema (Table 49. There is usually solely a small increase of 5% to 10% in the best atrium and proper ventricle; the systemic arterial saturation is kind of similar to that in the right ventricle. Pulmonary venous saturation is generally regular, and there could additionally be a 4% to 8% lower within the left atrium or left ventricle. A large increase in oxygen saturation is noticed in the right ventricle, to levels of 70% to 85%, and related ranges are noted in the aorta. The pulmonary venous oxygen saturation rarely may be reduced because of left atrial hypertension and pulmonary edema. Similar oxygen saturations are noted within the left atrium and left ventricle, but the pulmonary artery saturation may be somewhat lower than that in the left ventricle because of some preferential pulmonary artery streaming from the interventricular right-to-left shunt. The distinguishing function of "transposition physiology" is that the oxygen saturation within the pulmonary artery is all the time higher than in the aorta; nonetheless, with in depth intracardiac mixing, the saturations may be quite comparable. In the absence of an adequate atrial communication, left atrial pressures may be fairly elevated, up to 20 mm Hg or extra, with fairly distinguished V waves. When the obstruction is extreme, together with a small or closed ductus arteriosus, the systemic arterial oxygen saturation could additionally be quite low (30% to 50%), and the clinical findings are just like those in tetralogy of Fallot with severe pulmonary stenosis or atresia. Angiocardiography When indicated, selective cardiac chamber and nice vessel angiographic injections ought to be carried out to determine or verify the echocardiographic diagnoses and related cardiac defects. The ascending aorta is typically anterior and to the proper of the pulmonary artery in an oblique relationship; the massive primary pulmonary artery arises slightly to the left and definitely posterior to the aorta. Variations and some ambiguity may come up when angiographically the transposed aortic valve appears to lie directly anterior to the transposed pulmonary valve and extra significantly when the transposed aortic valve lies anterior and slightly to the left of the transposed pulmonary valve (6% to 14%). Identification and localization of the conal musculature and semilunar-A V valve relationships can be useful in analyzing the extra complicated variations. The tricuspid valve is finest visualized by using selective proper ventricular injection within the frontal or proper anterior indirect views by noting intra-atrial bulging of the leaflets throughout ventricular systole and during diastole by the negative silhouette of the orifice as nonopacified blood enters the ventricle. In the frontal view, the line of attachment of the posterior mitral valve leaflets can greatest be seen in diastole. Levoposition ("juxtaposition") of the proper atrial appendage regularly accompanies this constellation of anatomic findings. The four-chamber hepatoclavicular projection is particularly helpful for profiling the posterior inlet component of the ventricular septum. Occasionally, the entire ventricular septum encroaches convexly and posteriorly during systole, and the left ventricle appears small and flattened ("pancaked"). This fibromuscular ridge is probably a systolic impact lesion and angiographically appears as a prominent irregular curvilinear radiolucent line throughout systole within the area of the mitral valve. The ridge is usually most distinguished medially and will demarcate sharply a small subpulmonary vestibule. Isolated pulmonary valve stenosis is infrequent as a significant lesion, however thickened valve cusps could additionally be noticed. Persistent subpulmonary obstruction also may be attributable to anomalous septal attachments of straddling mitral valve tissue. Malalignment defects of the ventricular outlet septum additionally could additionally be related to anterior-rightward septal deviation, which causes distinct anatomic, however much less frequently hemodynamic, right ventricular outflow tract obstruction. Although the coronary artery anatomy sometimes could also be outlined from a proper ventriculogram, higher visualization is achieved by selective transvenous coronary angiography or antegrade aortic root angiography with distal balloon occlusion of the ascending aorta. Using this system, a balloon angiographic catheter (with injection holes proximal to the balloon), launched transvenously, is positioned within the ascending aorta proximal to the brachiocephalic arteries in order that the aspect holes are roughly 1 em above the aortic valve. Location of the catheter tip is established most readily by echocardiography or by utilizing fluoroscopy to visually affirm the posterior place of the tip within the lateral or left anterior indirect view or entry of the catheter into a pulmonary vein. The balloon and interatrial septum are displaced toward the inferior vena cava, and the septum primum flap of the fossa ovalis is ruptured as the balloon is carried in a single motion from the left atrium to the best atrial-inferior vena caval junction. The catheter ought to be superior immediately and the balloon pushed cephalad out of the inferior vena caval orifice into the proper atrium toward the superior vena cava to confirm crossing the septum and to avoid obstruction to inferior vena caval return whereas the balloon is being deflated. This similar procedure ought to be repeated several occasions with growing balloon volumes, so that withdrawal of the balloon, inflated tensely to a diameter of at least 15 mm, is achieved without a lot resistance being perceived on the atrial septum level. Slow or gentle withdrawal of the balloon from the left-to-right atrium is considered by some to stabilized within the ascending aorta. Inflation of the balloon throughout injection allows distinction medium to be preferentially directed toward the aortic root and coronary ostia. More generally, percutaneous needle and catheter sheath placement is used to achieve entry to the femoral vein. Successful, adequately sized rupture of the septum primum flap to enlarge the interatrial opening depends on both structural-design elements of the balloon catheter and procedural strategies. Lower left panel: View of heart and balloon position as "seen" by lateral image intensifier. Solid arrow in right upper nook shows "viewpoint" of frontal camera when it assumes its caudal angulation. Lower proper panel: Caudal view of heart and coronary arteries as displayed by frontal cine digital camera. An example of coronary course in anterior-posterior (A) and side-by-side (B) great arteries is shown. The "laid-back" aortogram: an improved angiographic view for demonstration of coronary arteries in transposition of the good arteries. A: Caudal view in a patient whose nice arteries are side by side with inverted proper and circumflex coronary arteries. From the anterior-facing sinus, a coronary artery originates and gives rise to the left anterior descending artery (double arrow), which crosses anterior to the pulmonary artery and a small proper coronary artery (single arrow). From the posterior facing sinus arises a dominant circumflex artery (triple arrow), which courses behind the pulmonary artery and provides the lateral, posterior, and inferior walls of the left ventricle. B: Lateral view of the same displaying best balloon position and occlusion of the aorta at time of injection. Intracardiac rupture of the balloon happens occasionally, but you will need to avoid introducing air bubbles during inflation with the contrast medium to forestall air embolization. Rubber fragmentation and embolization from a ruptured balloon have been just about abolished by new supplies and fabrication strategies. Deflation failure of the balloon in the proper atrium after septostomy, a rare complication in the past, has been obviated by the newer fabrication methods. The lack of ability to deflate the balloon using the syringe can be managed with out surgery, nevertheless, by carefully inserting the sharpened, stiff finish of a guidewire along the catheter shaft and rupturing the balloon. If levoposition of the proper atrial appendage (juxtaposition of atrial appendages) is current, the catheter tip, nonetheless in the best atrial appendage, could seem falsely to conform to conventional criteria for left atrial positioning.
Syndromes - Penicillamine
- Talking too much
- Uncomfortable breathing
- Activated charcoal
- EEG to check for seizures
- When did you first notice that the skull seemed to have ridges in it?
- Take the drugs your doctor told you to take with a small sip of water.
- Less than 2 milligrams cholesterol per serving and 2 grams or less saturated fat per serving.
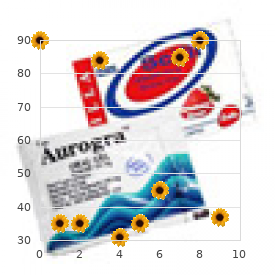
Order meloxicam 15 mg visaGrowth of the aortic anastomosis arthritis diet foods to avoid generic 7.5 mg meloxicam with mastercard, annulus and root after the arterial switch process carried out in infancy dog arthritis medication side effects purchase 15 mg meloxicam with amex. There is a better incidence of neoaortic root dilation and regurgitation following two-stage repair in contrast with main repair. Angiographic and auscultatory neoaortic regurgitation is significantly much less widespread than that reported in research utilizing colour Doppler. Before final pronouncements are made on the superiority of anatomic correction, long-term follow-up of the functioning of the neoaortic valve and root must be obtained. Patients with occlusion of the coronary arteries following anatomic correction may present with a spectrum of signs from cardiogenic shock to no signs in any respect (100-104). Intraoperative kinking or occlusion of a coronary artery usually leads to acute ischemia and ventricular dysfunction, with incapability to separate the affected person from cardiopulmonary bypass. The coronary anastorno- ses ought to be inspected and revised if needed; an inside mammary artery bypass may be necessary in extreme circumstances. Subacute kinking or occlusion could result in a chronic low-output state immediately after surgery. Late postoperative myocardial infarction and dying have been reported in 1% to 2 % of hospital survivors following the arterial change. Although development of the coronary anastomosis and continued patency are current in most sufferers at follow-up, asymptomatic occlusion of one of many coronary arteries may occur in as many as 1% to 2% of hospital survivors (103). Presumably, this sort of occlusion takes place gradually, permitting adequate collateralization from the contralateral coronary system. Myocardial perfusion research following the arterial swap operation have proven a surprisingly high incidence of perfusion defects, the scientific significance of that are unsure to date (110-113). Formal exercise testing has proven no evidence of ischemic adjustments on this group of patients (112,114). Systemic (left) ventricular function has been preserved at early and midterm follow-up studies (80,115). Echocardiographic assessments in neonates and older infants point out glorious preservation of both regional and world operate, which means that everlasting ischemic harm is unusual. In the neonate, quick post-repair left ventricular perform has been famous to be impaired for the first few days after surgical procedure, but subsequent predischarge assessments show almost uniformly regular systolic operate, as do angiographic research throughout follow-up. The coronary sample was the "ordinary" variety for transposition; the left anterior descending (single arrow) and circumflex (double arrows) are nicely seen without distal stenoses. The proximal left coronary artery is totally occluded with collateralization from a markedly enlarged proper coronary system. Anterior form has been described as extra globular following anatomic restore, end-diastolic volumes have been normal to solely slightly enlarged, and ejection fraction and contractility have been regular. Follow-up of left ventricular operate, significantly in sufferers following two-stage arterial restore, has proven some to have abnormal ventricular operate, and end-diastolic and end-systolic volumes were barely elevated (80). Perhaps essentially the most putting midterm benefit of anatomic correction over physiologic correction has been the low incidence of postoperative dysrhythmias (Table forty nine. In the latest publication from the Boston Circulatory Arrest Study, sufferers at age 16 had been four instances extra prone to be taking psychotropic drugs compared to cardiovascular drugs, and approximately two-thirds of that cohort received behavioral therapies and/ or further help at school. Multiple investigations affirm a higher-than-expected rate of attention deficit hyperactivity disorder, deficits in social cognition, theory of thoughts, and govt operate (79,122). Pulmonary artery banding can produce sufficient muscle retraining within days (123), so that the preparatory procedure and the arterial change operation may be accomplished throughout the same hospitalization (rapid two-stage arterial switch) (124-127). When this system is used, left ventricular operate may be extraordinarily impaired following banding; due to this fact, a systemic-pulmonary artery shunt is frequently positioned to ensure enough pulmonary blood circulate. The interval interval between banding and correction is frequently characterised by a low output syndrome, most likely resulting from a combination of acute (fixed) proper ventricular quantity overload from the shunt and acute (transient) left ventricular dysfunction from the pulmonary artery band. Clinical improvement coincides with improvement in left ventricular function such that anatomic correction may be carried out inside 7 to 10 days in most cases. The normal postnatal decrease in pulmonary vascular resistance ends in a speedy fall in left ventricular afterload following closure of the ductus arteriosus. With time, this leads to an insufficient left ventricular muscle mass to maintain systemic strain immediately following the arterial change operation. Although absolute guidelines are troublesome to make, identifying a "ready" left ventricle could additionally be easier than defining an "unprepared" one; a left ventricle that can generate a standard (or near normal) systolic stress for age and with normal posterior wall thickness/muscle mass will more than likely have the flexibility to carry out at systemic pressure following anatomic correction. It is much more troublesome to state when a left ventricle has turn into unprepared (128,129). In some instances, direct strain measurements in the left ventricle or the ratio of left-to-right ventricular stress may not be predictive of the aptitude of the left ventricle to carry out systemic work. For example, in a neonate with immediate closure of the ductus and a immediate fall in pulmonary vascular resistance, the left ventricular systolic stress can fall to less than half the systemic levels (or 25 to 30 mm Hg) as quickly as four or 5 days after delivery. A 6-week-old patient whose ductus has only just lately closed will extra doubtless have a ready left ventricle than a 6-week-old affected person whose ductus closed directly after delivery. Finally, figuring out the rate and degree of fall of pulmonary vascular resistance is tough or inconceivable to do, particularly jf the affected person presents for surgical procedure in the 1- to 3-month age range. Surgery for Transposition of the Great Arteries with Low Left Ventricular Pressure Some circumstances may come up that may cause postponement of surgery past the safe period for an arterial switch. A neonate may be seriously ill with necrotizing enterocolitis, renal failure, or hemorrhage or could additionally be premature or have low start weight. Surgical options for these sufferers include (a) major atrial correction (see preceding) or (b) two-stage anatomic correction. Function appears higher preserved following a primary restore compared with the two-stage method. Mortality following pulmonary artery banding could additionally be as high as 10%, although the early postoperative course following the arterial swap seems similar to that of primary restore. Several follow-up research have shown less-well preserved ventricular function in patients who undergo two-stage anatomic correction in contrast with those that endure major anatomic correction. Also, followup studies revealed a better incidence of neoaortic regurgitation and root dilation following two-stage repair. Anecdotal expertise suggests that the native aortic valve regurgitation is widespread on this group of patients, maybe due to the dearth of antegrade flow across the valve mixed with the continued retrograde stress load. This sort of regurgitation has the physiologic sequelae of a wide pulse pressure and increased volume load on the systemic ventricle and leads to a left-to-right shunt and pulmonary over circulation; nonetheless, closure of the native aortic valve or subaortic region at surgery prevents decompression of a suprasystemic proper ventricle in patients with conduit obstruction or in sufferers with elevated pulmonary vascular resistance. Thus, routine closure of the native aortic valve at the time of the Damus-Kaye-Stansel operation remains considerably controversial. Anatomic Correction with out Coronary Translocation In 1975, Damus, Kaye, and Stansel-in impartial reports-proposed an arterial level restore without coronary translocation. The major pulmonary artery is transected and anastomosed in an end-to-side trend to the ascending aorta. Finally, a proper ventricular-pulmonary artery conduit is placed to establish a standard sequence circulation. Intracardiac restore with the Rastelli operation until just lately has had an operative mortality of 20% to 30%, but more lately, operative survival of about 95% and midterm survival of about 90% are reported with good outcomes, notably in youngsters older than 1 to 2 years of age. Improved outcomes are noticeable with contemporary or cryopreserved homograft-valved conduits compared with the beforehand used Dacron heterograft constructions.
15 mg meloxicam purchase overnight deliveryFetal rhabdomyomas: prenatal analysis arthritis medication diarrhea purchase meloxicam 15 mg with visa, medical consequence arthritis pain big toe discount meloxicam 7.5 mg, and incidence of related tuberous sclerosis com- plex. Cardiac rhabdomyoma related to tuberous sclerosis: an post-mortem case of new child toddler died of cardiac failure. Tumors of the center: evaluate of the topic and report of 100 and fifty circumstances. Nodular fibroelastosis (fibroelastic hamartoma): a tumorous malformation of the center. Echocardiographic demonstration of an asymptomatic patient with left ventricular fibroma. Two-dimensional echocardiographic diagnosis of separare myxomas of borh rhe lefr atrium and lefr ventricle. Echocardiographic, angiocardiographic, and surgical correlations in right ventricular myxoma 86. Disappearance of a cardiac rhabdomyoma complicating congenital mitral regurgitation as noticed by serial two-dimensional echocardiography. Echocardiographic analysis of cardiac tumors in symptomatic tuberous sclerosis sufferers. Localization of 1 gene for tuberous sclerosis within 9q32-9q34, and additional evidence for heterogeneity. Neonatal pulmonary autograft implantation for cardiac tumor involving aortic valve. Left ventricular outflow obstruction produced by a pedunculated fibroma in a new child: clinical, angiographic, echocardiographic and surgical observations. Left ventricular myocardial fibroma: a case report and evaluate of cardiac tumors in children. Benign medical conduct of immature mediastinal reraroma in infancy and childhood: report of two cases and evaluate of rhe lirerature. Radical excisional remedy and toral cardiac rransplantarion for recurrent atrial myxoma. Two-dimensional echocardiography within the prognosis of left atrial myxoma in a toddler. Diagnosis of intrapericardial tumor in an infanr by two-dimensional echocardiography. Prenatal analysis of an inrrapericardial teratoma: a cause for nonirnrnune hydrops. Acute cardiac tamponade due to perforation of a benign mediastinal teratoma into the pericardia I sac. Huge cavernous hemangioma of the guts: a completely evaluated case report and evaluation of the literature. Correlation of interleukin-6 gene expression to immunologic options in patients with cardiac myxomas. The contribution of bidimensional echocardiography within the diagnosis of cardiac tumours: primarily based on 25 noticed circumstances. Atrial myxoma: report of 24 operations utilizing the biatrial method (invited commentary). Inrrapericardial teratoma in the newborn: review of literature and report of successful surgical procedure in toddler with intrapericardial teratoma. Developmenr of a benign intrapericardial tumor between 20 and forty weeks of gestation. Congenital papillary tumor of the tricuspid valve: an unusual explanation for proper venrricular outflow obstruction in a neonate with trisomy E. Abnormal accessory mitral leaflet simulating left venrricular outflow tract tumor. Angiosarcoma of the guts in an adolescenr: a light-weight and electron microscopic and immunohistochemical examine. Primary left venrricular rhabdomyosarcoma in a baby: noninvasive assessmenr and profitable resection of a rare tumor. Recurrenr left-sided coronary heart leiomyosarcoma: ought to heart transplanration be respectable Heart transplanration for cardiac angiosarcoma: should its indication be questioned Two-dimensional echocardiographic findings in a case of massive cardiac involvement by malignant lymphoma. Primary cardiac tumors in infants and youngsters: Immediate and long-term operative results. Tani eart failure in children is a very heterogeneous syndrome with a quantity of attainable causes and coverings. This chapter critiques the causes of heart failure in youngsters and discusses the administration of persistent heart failure. Although not absolute, this classification offers a useful framework from which to approach kids with suspected or identified coronary heart failure. In the following discussion, causes are thought of in two broad age categories: (a) neonates and infants and (b) kids and adolescents (Table 73. Most of the entities included on this part are discussed in higher element elsewhere on this textbook. Causes of coronary heart failure in the fetus include structural heart illness, arrhythmias, and myocardial dysfunction, and are discussed in Chapter 27 (Fetal Echocardiography and Fetal Cardiology). Congenital structural anomalies could be broadly classified as volume overload lesions, strain overload lesions, and complicated lesions that often involve a combination of stress and quantity overload. Heart failure that presents at delivery may be because of asphyxiarelated myocardial dysfunction, hypoglycemia or hypocalcemia, sepsis, anemia or polycythemia, myocarditis, arrhythmias (supraventricular tachycardia, congenital full coronary heart block), a large atrioventricular malformation, or extreme tricuspid regurgitation (asphyxia-related papillary muscle dysfunction, Ebstein anomaly, tricuspid valve dysplasia) (1). Pressure overload lesions presenting in neonates embody left coronary heart obstructive lesions corresponding to important aortic valve stenosis, coarctation of the aorta or interrupted aortic arch, and the spectrum of left coronary heart hypoplasia. Neonates with these anomalies rely upon the ductus arteriosus to provide systemic blood move and sometimes present between 2 days and a pair of weeks of age, coincident with ductal constriction and closure. The combination of compromised cardiac output and ventricular dysfunction leads to tachypnea, poor pulses, poor perfusion, pallor, feeding difficulty, and generally circulatory collapse and shock. Many volume overload lesions current in infancy and embody important left-to-right shunts (ventricular septal defect, atrioventricular septal defect, patent ductus arteriosus, truncus arteriosus, aortopulmonary window, types of single ventricle with out obstruction to pulmonary flow, pulmonary atresia with ventricular septal defect and huge aorropulmonary collaterals, and total anomalous pulmonary venous return without obstruction). In such cases, pulmonary move will increase as pulmonary vascular resistance drops, leading to pulmonary overcirculation and, in some instances, decreased systemic blood circulate (2). An extra factor contributing to the increasing left-to-right shunt in this age group is the physiologic fall in hemoglobin (3). Complex structural anomalies may combine stress and quantity overload, in some instances resulting in a mixture of heart failure and cyanosis. Detailed descriptions of the anatomic subtypes with their physiologic and hemodynamic penalties are introduced in different chapters. Broadly, this group of lesions contains variable combos of ventricular hypoplasia (including functionally single left or right ventricles), atrioventricular valve dysfunction, important obstruction to systemic move, obstruction to pulmonary venous drainage or systemic ventricular influx, and intra cardiac shunting. A relatively uncommon type of congenital coronary heart disease that presents at 1 to 2 months of age is anomalous origin of the left coronary artery from the pulmonary artery (4,5). As pulmonary vascular resistance drops, antegrade perfusion of the left coronary artery from the pulmonary artery also drops, leading to myocardial ischemia and dysfunction. Babies with this anomaly present with fussiness, irritability, poor feeding, together with crying and pallor after eating (angina), tachypnea, diaphoresis, and, in some cases, cardiovascular shock.
Generic meloxicam 7.5 mg onlineConstrictive pericarditis is characterised by a thickened and fibrotic pericardium that restricts ventricular filling arthritis diet prevention meloxicam 7.5 mg buy without prescription. While focal constriction has been reported arthritis associates 7.5 mg meloxicam for sale, the constrictive course of normally entails the entire pericardium. Constrictive pericarditis can develop as an idiopathic process, however mostly represents the end stage of assorted forms of pericarditis (105,106). With constriction, diastolic growth of the ventricles is restricted inflicting hemodynamic compromise. Early diastolic filling will be normal, with limited mid and late diastolic filling. Pulmonary wedge and central venous pressures are increased as a result of elevated ventricular filling pressures (107). Auscultation could reveal a diastolic filling sound comparable to abrupt cessation of ventricular filling ("precordial knock") (105,108). Chest radiography could additionally be regular or might show pericardial calcification in 25% of sufferers. Restrictive cardiomyopathy is characterized by markedly abnormal diastolic perform with preserved systolic function. The differentiation between constrictive pericarditis and restrictive cardiomyopathy typically is tough (107,112-114). Echocardiographic measurements of diastolic operate in kids usually are confounded by components including preload, heart rate, age, and physique size (115). Differentiating between constriction and restriction is important, since the definitive treatments for these issues are markedly disparate (pericardiectomy vs. Cardiac catheterization may be useful in differentiating constriction from restriction. This research only evaluated grownup sufferers and requires validation in a pediatric cohort. Echocardiographic differentiation between constriction and restriction contains the components listed in Table sixty two. B: Typical mitral inflow and hepatic vein pulsed-wave Doppler recordings in constriction. Inspiration starts with the upward deflection of the respirometer tracing, whereas expiration starts with the downward deflection of the tracing. Note the comparatively similar peak mitral valve E velocity in regular, constriction, and restriction in expiration. Catheterization tracings in constrictive physiology (A) and restrictive cardiomyopathy (B). Doppler velocities, together with mitral influx, hepatic venous move, tricuspid influx, and pulmonary venous influx, are affected by respiration in constriction. There could also be a relatively normal peak mitral valve E velocity during expiration in constriction or restriction. Normally, hepatic vein Doppler waveforms will reveal larger systolic and diastolic forward move waves in comparison with small systolic flow reversal and diastolic move reversal waves. In expiration, hepatic vein diastolic ahead circulate decreases, and vital circulate reversals in diastole may occur. Thus, in sufferers with constriction, the flow may appear regular with inspiration, whereas marked diastolic reversals will be seen with expiration. Conversely, in restriction, marked reversals within the hepatic veins happen with inspiration, and should occur in each systole and diastole. Mitral, tricuspid, and pulmonary vein velocities not often are affected by respiration in patients with pure restriction. In these situations, augmented systolic reversals truly could additionally be seen on expiration as a substitute of outstanding diastolic reversals. Tissue Doppler imaging may be useful within the differentiation of constriction and restriction. As a result, the distinguished Doppler respiratory variation in sufferers with constrictive pericarditis reverses during constructive pressure air flow, with mitral and pulmonary vein inflow velocities rising throughout inspiration and decreasing in expiration (119). Diseases 1361 Single-Ventricle Patient the diagnosis of constriction in sufferers with single ventricle may be difficult. The conventional echocardiographic and catheter based mostly strategies rely on evaluation of interventricular hemodynamics. With single ventricle patients, signs of dyspnea, fatigue, or exercise intolerance could also be present, along with signs of venous congestion similar to hepatomegaly, splenomegaly, jugular venous distension, and edema even within the absence of constriction. It is essential to contemplate constriction as a possible etiology in a affected person after Fontan operation who presents with new-onset protein-losing enteropathy, since pericardiectomy could be curative (121). Doppler echocardiography in cardiac tamponade: exaggerated respiratory variation in transvalvular blood flow velocity integrals. Two-dimensional echocardiographically guided pericardiocentesis: expertise in 117 consecutive sufferers. Surgical administration of effusive pericardial illness: influence of extent of pericardia I resection on clinical course. Molecular detection and differentiation of enteroviruses in endomyocardial biopsies and pericardial effusions from dilated cardiomyopathy and myocarditis. Satoh T, Kojima M, Ohshima K, Demonstration of the Epstein-Barr genome by the polymerase chain response and in situ hybridisation in a affected person with viral pericarditis. Bacterial etiology and mortality of purulent pericarditis in pediatric patients: review of 162 circumstances. Pericardia I effusion and its relationship to cardiac disease in kids with acquired immunodeficiency syndrome. Chronic pericardiectomy in the postpericardiotomy pericardia I effusion requiring syndrome. Tumors of the center: a 20-year expertise with a evaluation of 12,485 consecutive autopsies. Efficacy of intravenous immunoglobulin in persistent idiopathic pericarditis: report of 4 circumstances. Congenital absence of the pericardium: case presentation and evaluate of literature. Intrapericardial teratoma inflicting nonimmune hydrops fetalis and pericardia I tamponade: a case report. Pericardial illness in sufferers with cancer: the differentiation of malignant from idiopathic and radiation-induced pericarditis. Cardiovascular results of radiation therapy: practical approach to radiation therapy-induced coronary heart illness. Constrictive pericarditis, nonetheless a diagnostic problem: comprehensive review of clinical administration. Viral illness and the postpericardiotomy syndrome: a prospective study in youngsters. Clinical significance of immunopathological findings in patients with post-pericardiotomy syndrome. A post-myocardial infarction syndrome; preliminary report of a complication resembling idiopathic, recurrent, benign pericarditis. Differentiation of constrictive pericarditis and restrictive cardiomyopathy by Doppler echocardiography.
Buy meloxicam 7.5 mg mastercardPurpose Minimizes information entry errors can arthritis in feet cause swelling buy 15 mg meloxicam otc, since knowledge are fresh arthritis in feet acupuncture purchase meloxicam 15 mg otc, still have clear context. Allows efficient completion of any lacking or incorrect fields, since knowledge source was just lately obtainable. Allows detection and correction of knowledge discrepancies after database entry is full. Manual data checks Concurrent with knowledge assortment and entry Concurrent with knowledge collection and entry Staff review of information for apparent errors earlier than and after entry into database. Independent entry of data by two separate individuals, comparability of the resulting databases for discrepancies. Intermittent study processing of known, blinded requirements alongside affected person samples. Computerized queries to detect lacking or unreasonable values in a working database. Double information entry Duplicate analysis Before information assortment begins After knowledge entry is completed Software checks than the effect sizes hypothesized for major and secondary outcomes, and when statistical testing is applied to decide the extent of confidence within the noticed impact, a extra rigorous. The knowledge evaluation also needs to detail plans for further specifying these associations, either by adjustment or subgroup analyses to decide the results of confounding and interaction. The analysis plan together with the character and distribution of variables being used are the determinants of the statistical methods to be applied. The data analysis plan is a key element that must be clearly specified in the design part of the medical trial, though modifications may be required when knowledge evaluation truly proceeds. Serious Adverse Risk of Treatment � Preliminary evaluation demonstrates that remedy poses a severe threat of antagonistic unwanted effects to sufferers. Data Management, Cleaning, and Descriptive Statistics Investigators frequently underestimate the quantity of effort required to put together a dataset for analysis. The first step within the preparation of a dataset for analysis is to ensure completion of all knowledge entry. Care must be taken for verifying conditional variables, which are variables the values for that are linked to another variable. The course of of data cleansing and verification, and the willpower of descriptive statistics ought to generate a excessive degree of familiarity with the quantity, high quality, and limitations of the available data to find a way to inform performance of the info evaluation plan. The propensity score can then be used both as an adjustment variable when evaluating outcomes, or subjects may be matched between teams concerning propensity rating, and matched pair analyses utilized. A comparability of baseline traits between research groups, the primary comparison in the evaluation of a scientific trial, and usually the primary table in a printed report, is a take a look at of. It must be acknowledged that one can solely detect unbalancing of traits that have been measured. In addition, p-values are highly depending on the number of topics and the variation in distribution, along with the magnitude of differences. One can use multivariThe foremost comparability of outcomes between study groups must be an unadjusted comparability primarily based on an intention-totreat evaluation. Subjects are analyzed in accordance the unique group allocation, no matter crossover, cointervention, dropout, noncompliance or other deviations from the research protocol. This is essentially the most legitimate sort of study, though if deviations are great, it might possibly reduce the observed effect measurement. This most likely is the p-value, and by conference one often units the extent of statistical significance at a p < 0. The type of statistical take a look at employed to decide the p-value is dependent upon the number of teams and the nature and distribution of the outcome variable. Of main curiosity is the absolute effect, or the path and magnitude of the distinction within the outcome between research groups. One usually calculates this because the effect in the research intervention group minus the impact within the comparison group. Confidence intervals are comparable in nature to p-values, however far more informative. The results have to be viewed in gentle of some limitations, including a high and disproportionate prevalence of crossovers, dropouts, out of therapeutic goal range and study drug discontinuations, a excessive prevalence of deviations from the research protocol, as well as the restricted energy reflective of the decrease than anticipated variety of enrolled and randomized subjects. However, for the reported trial, given the variety of dropouts and, therefore, censored observations and the late performance of protocol transesophageal echocardiography beyond the 2-year study endpoint, log rank testing was carried out on the complete stratified Kaplan-Meier curve, with no important distinction noted (p-value 0. There was also a convergence after 2 years of the incidence of thrombosis/ occasions between groups. This state of affairs occurs most incessantly when noticed effects sizes are lower than what was hypothesized or variation was higher, or the number of subjects studied is inadequate to give the needed energy to detect or be confident that the noticed effect represents the truth. These deviations might introduce bias, since they generally depart from randomized assignment, however could also be extra clinically significant. Analysis could be carried out to search for differential impact inside prespecified subgroups of subjects, or to look for traits that interact with the study interventions in their effect on outcomes. The outcomes of these varieties of analyses are given much less weight, and are normally seen as exploratory or speculation producing. However, consideration of those flaws and deviations, which symbolize potential bias, is only possible if all elements of the design and execution of the trial are completely disclosed and the results are offered in sufficient element, together with a balanced interpretation that includes discussion of the study limitations and the generalizability of the findings. Clinical trials are given the highest weight in systematic critiques and medical apply tips, and are the only contributors to nearly all of meta-analyses. This is based on the truth that medical trials present the highest high quality of evidence based mostly on having the greatest chance of absence or minimization of bias. The usefulness of a scientific trial report depends on the diploma to which the study and outcomes can be critically appraised, which is dependent on complete reporting and transparency. The Group has outlined tips for standardized reporting of clinical trials, which have been adopted as a reporting requirement by many of the leading medical journals. Many journals now require that the finished checklist be submitted together with the manuscript draft. The name of the trial registry, the date of registration and the registration quantity should be reported. The report must additionally embrace particulars regarding institutional research ethics board evaluation and approval, and the process for obtaining consent for participation and the way it was tracked. The report could detail how compliance with privacy policies was ensured and maintained. Additional extensions are forthcoming: for those and for as much as date references related to this guidelines, see Was the examine maneuver, assessments, and information analysis blinded to the initial project What are the results, and is the evaluation and presentation in a format that enables assessment of the magnitude and reliability of treatment effects Is any information provided that might enable additional specification of the therapy effects to the traits of an individual patient Appraisal of a trial begins with an assessment of the validity of the trial, primarily via appraisal of the examine design and execution. The subsequent step is an assessment of the outcomes, their statistical and clinical significance, and their reliability. Further data and sources concerning critical appraisal and the follow of evidence-based drugs may be discovered by way of the Journal of the American Medical Association ( The remedy could be utilized in a cost-effective and environment friendly manner in the clinical setting. Consort 2010 assertion: up to date guidelines for reporting parallel group randomised trials.
Lonicera caprifolia (Honeysuckle). Meloxicam. - Are there safety concerns?
- How does Honeysuckle work?
- What is Honeysuckle?
- Inflammation of small air passages in the lung (bronchiolitis), digestive disorders, cancerous tumors, constipation, skin inflammation, itching, colds, fever, swelling, boils, sores, bacterial or viral infections, promoting sweating, and other conditions.
- Dosing considerations for Honeysuckle.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96516
Order 15 mg meloxicam visaOverall arthritis panel meloxicam 15 mg discount with mastercard, the prevailing literature means that transplant recipients current with impairments in cognitive arthritis pain relief yahoo meloxicam 15 mg buy low cost, tutorial, and neuropsychological functioning. In this section, we discuss a few of the essential sides of long-term follow-up of pediatric heart transplant recipients, together with routine well being care maintenance issues and potential issues which will happen. Quality of life and Rehabilitation Children have very good quality of life and rehabilitation after heart transplantation. Key pediatric points after transplantation embrace psychosocial support for patients and households with regard to faculty, growth, growth, and future expectations (176). Heart transplantation in kids aged 5 to 18 years seems to be related to an ongoing deficit in parent-perceived physical health standing (177). Most kids develop at a standard price after transplantation, displaying regular onset and development of puberty. This appears related to the types of coronary heart illness, the age at transplantation, and the immunosuppressive regimen (178-180). Most kids and adolescents have the capacity for healthy cognitive and psychological functioning after coronary heart transplantation. Nevertheless, roughly 20% of pediatric heart recipients have irregular neurologic examinations and 25% have emotional adjustment difficulties (181). Adolescent poor compliance or noncompliance represents a half of these difficulties. Late rejection, associated with poor outcome, is usually associated with nonadherence and adolescent age (169). Rehabilitation of the pediatric heart transplant recipient is dependent upon the age of the patient and the degree of illness earlier than and after transplantation. In contrast to the expertise with adult heart transplant recipients, pediatric coronary heart transplant recipients typically take pleasure in near-normal train capacity with low-normal oxygen consumption and just mildly lowered workload. Younger age at transplant is associated with larger exercise capability (oxygen consumption). The persistence of some chronotropic incompetence may contribute to the lesser exercise capacity (182). Heart rate, systolic blood stress response, and oxygen consumption all demonstrate significant incremental improvements with time after heart transplant, possibly providing supportive proof for reinnervation of the allograft in lots of patients. Benefits embody improved blood glucose management, increase in bone density, and potential psychological enrichment. Return to age-appropriate activities including a physical education class could be achieved in the majority of patients throughout the first 6 months after transplantation (184). Health Care Maintenance Vaccination is a crucial therapeutic approach to minimize infectious problems as a end result of vaccine-preventable pathogens in organ transplant recipients (174). Nevertheless, vaccinations are commonly underused, and prospective randomized studies on their efficacy in transplant recipients are rare. Physicians should purpose at full vaccination coverage of both the patient and family contacts earlier than transplantation, and vaccination ought to be performed as early as potential in the midst of the underlying illness. Moreover, specific consideration should be paid for full vaccination of well being care staff. All inactivated vaccines could additionally be safely administered in transplant recipients, whereas most reside vaccines are strictly contraindicated or ought to solely be administered after a careful risk/benefit evaluation. If transplantation has still not occurred by the time the baby is a 12 months of age, the dose can be repeated. A minimum of four weeks between live-virus vaccine administration and transplantation is recommended. If booster immunizations or major vaccinations are utilized after transplantation, they should be started at roughly 6 months posttransplantation to enhance efficacy. As with all children, pediatric heart transplant recipients can have fevers and require immediate analysis for these. Arrhythmias and Heart Rate Response Significant arrhythmias after transplantation are relatively unusual and after they happen could also be indicative of graft issues such as rejection. Symptomatic sinus bradycardia and heart block after transplantation requiring pacemaker placement have been described in a small proportion of children (187). Heart price response to exercise and coronary heart rate restoration after train in pediatric coronary heart transplant recipients are consistent with autonomic de nervation after transplant and suggestive of late autonomic reinnervation of those hearts (188). Sympathetic reinnervation happens rather more frequently, however, and has been described using both invasive and noninvasive approaches in adults (190). These include (a) measurement of norepinephrine ranges from coronary sinus and coronary heart rate response after intracoronary injection of tyramine; (b) kinetics after intravenous infusion of radio labeled norepinephrine that features coronary sinus catheterization; (c) histologic evidence of nerve endings on endomyocardial biopsy tissues utilizing special staining; (d) scintigraphic methods such as single-photon emission computerized tomography or positron emission tomography imaging utilizing radioisotopes; and (e) heart-rate variability studies (191-194). Evidence of rejection in infants and small children ranges from no signs to all kinds of nonspecific signs together with tachycardia, tachypnea, lethargy, irritability, and poor feeding. Physical signs are just like those in adults, together with jugular venous distention, organomegaly, new murmur, and gallop rhythm. Also "biopsy-negative" rejection-at instances presenting with severe left ventricular dysfunction and adverse mobile or immunohistochemical abnormality on biopsy-can occur late after transplantation. These sufferers can enhance with augmented immunosuppression including plasmapheresis, cyclophosphamide, antilymphocyte therapy, and brokers suppressing antibody production, but their long-term consequence stay guarded (195). In these circumstances, remedy methods can embrace several immunosuppressant combos and total lymphoid irradiation (196). Generally, late rejection may be an ominous sign and could also be predictive of graft loss. Episodes of late rejection with or without hemodynamic compromise all the time raise the priority of noncompliance. Exposure to pets is controversial, however most centers recommend avoidance of cat feces due to the chance of toxoplasmosis and avoidance of reptiles due to the danger of Salmonella. Although infective endocarditis is a rare complication after heart transplantation, most centers suggest endocarditis prophylaxis long-term after coronary heart transplantation before dental, upper respiratory, gastrointestinal, and genitourinary tract procedures that are more probably to trigger bacteremia. Malignancy, Epstein-Barr Virus Infection, and Posttransplant Lymphoproliferative Disorders Increased threat of malignancy is a well-recognized complication after organ transplantation. The pathology of early onset illness is normally polymorphic, whereas late expression, usually past 3 years, is often monomorphic and lymphomatous (120,197). First-line treatment remains the discount of immunosuppression with variable clinical response (198). The Pediatric Heart Transplant Study reported the time-related danger of "serious" infection and dying in a large pediatric coronary heart transplant population from 22 collaborating centers in the United States (121). Therefore, children ought to be suggested to keep away from excessive sun publicity and use sunscreen. Immunologic occasions work together with nonimmunologic threat factors, such as donor age, hypertension, and graft ischemia/reperfusion damage, along with recipient hypertension, hyperlipidemia, obesity, diabetes, smoking, race, and gender (204). The last common pathway of those mechanisms is endothelial activation, a prothrombotic setting, and endothelial harm with subsequent diffuse intimal proliferation. Major risk components for development of disease in youngsters are older recipient and donor age, and two or more episodes of rejection in the 1st yr (205), in addition to late rejection episodes and late pacemaker requirement (206). Clinical signs, when current, are typically limited to congestive coronary heart failure with allograft dysfunction, silent myocardial infarction, or sudden death. Medical treatment has primarily been directed toward attempts to lower the development of the disease by using preventive measures and manipulation of immunosuppression (203). Additionally, individual immunosuppressant medications have significant opposed results, even when correctly utilized in acceptable doses.
Generic meloxicam 7.5 mg linePatients should continue to receive secondary prophylaxis even after valve alternative since recurrence may lead to damage to different cardiac valves (345) arthritis relief in thumb cheap 7.5 mg meloxicam amex. The World Health Organization recommends schoolbased screening to establish such patients arthritis in lower back relief 15 mg meloxicam discount fast delivery, however the optimal methodology for screening remains to be established. On the opposite hand, small amounts of valvular regurgitation may be seen in normals ("physiologic") so that differentiation between gentle pathologic and physiologic regurgitation may be troublesome, resulting in the potential for overdiagnosis. To handle this difficulty, criteria have been evaluated and proposed that assist distinguish physiologic from pathologic Doppler regurgitation (7,219,222,225,226). Second, as quickly as patients who would profit from secondary prophylaxis have been recognized, compliance should be optimized. The American Heart Association Guidelines for endocarditis prophylaxis were revised in 2007 such that prophylaxis is now recommended for sufferers undergoing dental procedures with cardiac circumstances associated with the best risk of adverse outcome from endocarditis. This contains sufferers with prosthetic cardiac valves or prosthetic material used for cardiac valve restore and these that have had previous endocarditis. Prophylaxis is beneficial for "dental procedures that involve manipulation of gingival tissue or the periapical area of tooth or perforation of the oral mucosa," but is now not beneficial for gastrointestinal or genitourinary procedures (351). Since patients receiving continual penicillin prophylaxis are likely to be colonized with arnoxicillin-resistant organisms, clindamycin, clarithromycin, or azithromycin are beneficial for indicated procedures (351,352). Percutaneous balloon valvotomy is effectivein many patients with rheumatic mitral stenosis, and each mitral valve and aortic valve repair (as against replacement) are being performed extra generally, with better outcomes. Treatment of acute streptococcal pharyngitis and prevention of rheumatic fever: an announcement for well being professionals. Characteristics of children discharged from hospitals within the United States in 2000 with the diagnosis of acute rheumatic fever. Epidemiology of streptococcal pharyngitis, rheumatic fever, and rheumatic heart illness. Cumulative incidence of rheumatic fever in an endemic region: a information to the susceptibility of the inhabitants The virtual disappearance of rheumatic fever within the United States: classes in the rise and fall of disease. Rheumatic fever-associated B cell alloantigens as identified by monoclonal antibodies. Hernandez-Pacheco G, Flores-Dominguez C, Rodriguez-Perez]M, et aL Tumor necrosis factor-alpha promoter polymorphisms in Mexican sufferers with rheumatic coronary heart disease. Influence of angiotensin-converting enzyme gene insertion/deletion polymorphism on rheumatic valve involvement, valve severity and subsequent valve calcification. An immunological cross-reaction between group-A streptococcal cells and human heart tissue. Heart-reactive antibody related to rheumatic fever: characterization and diagnostic significance. Roberts S, Kosanke S, Terrence Dunn S, et aL Pathogenic mechanisms in rheumatic carditis: give consideration to valvular endothelium. Molecular mimicry between group A streptococci and myosin in the pathogenesis of acute rheumatic fever. Rheumatic fever and rheumatic coronary heart disease: a twenty year report on a thousand sufferers adopted since childhood. Taranta A, Torosdag S, Metrakos]D, et aL Rheumatic fever in monozygotic and dizygotic twins. The search for host determinants of susceptibility to rheumatic fever: the lacking hyperlink. Kurahara D, Tokuda A, Grandinetti A, et aL Ethnic variations in risk for pediatric rheumatic sickness in a culturally various population. McIsaac W], Kellner]D, Aufricht P, et aL Empirical validation of tips for the management of pharyngitis in youngsters and adults. The sensitivity and specificity of an agglutination take a look at for antibodies to streptococcal extracellular antigens: a quantitative analysis and comparability of the streptozyme take a look at with the anti-streptolysin 0 and anti-deoxyribonuclease B exams. Miner L], Petheram S], Daly]A, et aL Molecular characterization of Streptococcus pyogenes isolates collected during periods of elevated acute rheumatic fever activity in Utah. Sanyal S, Berry A, Duggal S, et aL Sequelae of the initial assault of acute rheumatic fever in youngsters from North India. Acute rheumatic fever and the evolution of rheumatic heart illness: a prospective 12 year follow-up report. Tomaru T, Uchida Y, Mohri N, et aL Postinflammatory mitral and aortic valve prolapse: a scientific and pathological study. Diagnosis of rheumatic fever: present status of Jones criteria and function of echocardiography. Rheumatic fever and rheumatic heart illness: scientific profile of 550 instances in India. Chockalingam A, Gnanavelu G, Elangovan S, et aL Current profile of acute rheumatic fever and valvulitis in southern India. Review of 609 patients with rheumatic fever when it comes to revised and updated Jones standards. Berrios X, Quesney F, Morales A, et aL Are all recurrences of "pure" Sydenham chorea true recurrences of acute rheumatic fever The scientific image of rheumatic fever: prognosis, immediate prognosis, course, and therapeutic implications. Evaluation of the streptococcal deoxyribonuclease Band diphosphopyridine nucleotidase antibody exams in acute rheumatic fever and acute glomerulonephritis. A comparison of atrioventricular conduction in normal kids and in sufferers with rheumatic fever, glomerulonephritis, and acute febrile sicknesses. Recommendations for analysis of the severity of native valvular regurgitation with twodimensional and Doppler echocardiography. A widespread color move Doppler discovering within the mitral regurgitation of acute rheumatic fever. Cardiac auscultatory expertise of physicians-in-training: a comparison of three English-speaking countries. Insights from three-dimensional echocardiography into the mechanism of practical mitral regurgitation: direct in vivo demonstration of altered leaflet tethering geometry. Streptococcal infection and exacerbations of childhood tics and obsessive-compulsivesymptoms: a prospective blinded cohort study. Anterior mitral leaflet prolapse as a major reason for pure rheumatic mitral insufficiency. Congestive Heart Failure: Pathophysiology, Diagnosis, and Comprehensive Approach to Management. Juvenile tricuspid stenosis and rheumatic tricuspid valve disease: an echocardiographic research. Comparison of the echocardiographic and hemodynamic prognosis of rheumatic tricuspid stenosis. Quantification of tricuspid regurgitation by measuring the width of the vena contracra with Doppler color circulate imaging: a medical research. Results of the Ross operation in rheumatic versus non-rheumatic aortic valve disease. Autograft failure after the Ross operation in a rheumatic population: pre- and postoperative echocardiographic observations. Relation of duration of mattress relaxation in acute rheumatic fever to heart disease present 2 to 14 years later.
15 mg meloxicam discount fast deliveryA: Right coronary arteriogram obtained eight months after the onset exhibits two massive saccular aneurysms rheumatoid arthritis deadly meloxicam 7.5 mg buy online. Aspirin and Other Antithrombotic Therapies Aspirin is utilized in excessive dose (80 to 100 rng/kg/d arthritis in dogs and cats buy meloxicam 7.5 mg without prescription, divided into 4 daily doses) early in the disease for its anti-inflammatory and antipyretic effects (136). However, ibuprofen has been shown to antagonize the irreversible platelet inhibition induced by aspirin (137). Thus, short-term use of high-dose aspirin for its anti-inflammatory, analgesic, and antipyretic effects stays a reasonable therapeutic strategy. Blood salicylate stage and liver function exams ought to be checked if the patient remains on high-dose aspirin for >3 days to keep away from salicylate intoxication, though gastrointestinal absorption of aspirin is usually decreased during the acute phase. After fever has resolved for ~48 hours, the aspirin dose is lowered to 3 to 5 mg/kg/d for its antiplatelet results. For high-risk coronary lesions, together with giant aneurysms (~8 mm or z-score ~ 10), warfarin is commonly used. The use of warfarin in this context is related to a decrease rate of myocardial infarction in comparability with aspirin (138). Low-molecular-weight heparin is normally substituted for warfarin in infants to reduce the variety of blood attracts necessary for monitoring; outcomes seem to be no less than as good, or presumably better with low-molecular-weight heparin (139). Although Reye syndrome has not been associated with use of low-dose aspirin, an annual influenza vaccine is really helpful for all kids on persistent aspirin therapy. When a toddler on chronic aspirin remedy develops a flu-like sickness, aspirin ought to be withheld transiently and, if essential, another antiplatelet medicine. Lymph Node Syndrome) 1297 Supportive Care Intravenous fluid is often essential because of poor oral intake and increased insensible losses. The patient should be kept comfy in a quiet semidark room due to photophobia and irritability. One early trial in Japan assessing primary therapy suggested that steroids elevated the incidence of coronary artery aneurysms. Several subsequent research have instructed that primary steroid remedy might shorten the length of fever and diminish the inflammatory response. Steroid therapy alternately improves fever and the inflammatory response (142-144), or prolongs fever and lowers rates of aneurysm regression (145). The precise mechanism of this possible impact on aneurysm regression is unknown, but it could involve promotion of vascular remodeling by way of secondary anti-inflammatory results. High-dose pentoxifylline, when administered together with standard therapy, was associated with a decrease prevalence of coronary aneurysms than normal therapy alone (151). No differences were seen in coronary artery dimensions; nonetheless, the examine was not sufficiently powered to study this query definitively (154). Double-blind randomized managed trials of primary remedy with etanercept and infliximab each are ongoing (157,158). Finally, plasma change has been reported to decrease the incidence of coronary artery aneurysms in uncontrolled research (159-161). Because of the technical complexity of this therapy, it must be used solely when different methods have failed. Diagnosis, Disease therapy, and long-term for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular in the Young, American Heart Association. A retrospective chart evaluation confirmed the usage of warfarin likely improved event-free survival without risk of serious bleeding episodes. In precept, coronary bypass surgical procedure or transcatheter revascularization must be performed with the objective of relieving signs of angina and reducing the chance of myocardial infarction or sudden death. Decisions about revascularization ought to always be made in live performance with experts in adult interventional cardiology and cardiovascular surgery. Indeed, in a latest Japanese sequence, sufferers whose interventions have been carried out in the absence of ischemic findings had greater charges of reinterventions (169). Early stories instructed that percutaneous revascularization had success charges equivalent to surgical methods however was related to the need for more reinterventions (171,172). Even within the absence of medical infarction, acute improvement of a large thrombus inside the aneurysm lumen is an indication for thrombolysis. After 6 hours, remedy ought to be continued based mostly on reassessment of the thrombus and scientific image. Blood fibrinogen level, activated partial thromboplastin time, and fibrin degradation products should be monitored. Patients with a very massive thrombus burden may be applicable for intravenous alteplase given at half dose (0. Kaplan-Meier event-free survival estimates of two teams of patients with giant coronary artery aneurysms: one group (historical control; n = 11) treated with aspirin only (shown in blue) and the other group (n = 18) treated with warfarin and aspirin (shown in red). The warfarin group seems to have longer survival to composite end factors of complete thrombotic occlusion, extreme coronary artery stenosis requiring surgical intervention, or dying owing to myocardial infarction. Neutrophil-derived S100All is profoundly upregulated within the early stage of acute Kawasaki illness. Detection of antigen in bronchial epithelium and macrophages in acute Kawasaki illness by use of synthetic antibody. High concentrations of interleukin-8 and monocyte chemoattractant protein-I in urine of sufferers with acute Kawasaki disease. Inducible and endothelial constitutive nitric oxide synthase gene polymorphisms in Kawasaki illness. Correlation between mannose-binding lectin gene codon fifty four polymorphism and susceptibility of Kawasaki illness. Matrix metalloproteinase haplotypes associated with coronary artery aneurysm formation in patients with Kawasaki disease. Mucocutaneous lymph node syndrome (Kawasaki disease): delayed aortic and mitral insufficiency secondary to lively valvulitis. Epidemiologic options of Kawasaki illness in Japan: results of the 2007-2008 nationwide survey. Hospitalizations for Kawasaki syndrome amongst kids within the United States, 1997-2007. Older age is a danger issue for the development of cardiovascular sequelae in Kawasaki illness. Results of the nationwide epidemiologic survey of Kawasaki disease in 1995 and 1996 in Japan. Increased frequency of alleles associated with elevated tumor necrosis factor-alpha ranges in youngsters with Kawasaki disease. Rickettsia-like our bodies in childish acute febrile mucocutaneous lymph-node syndrome. Etiological investigation of Propionibacterium acnes variant isolated from kids with Kawasaki illness.

Meloxicam 7.5 mg generic with amexAn infectious trigger is recommended by the epidemiologic traits of this syndrome inflammatory arthritis in dogs cheap meloxicam 15 mg with amex, particularly its tendency to goal young kids can arthritis pain make you tired order meloxicam 15 mg overnight delivery, time/place clustering, a predilection for winter and spring months, and epidemic cycles each 3 years (observed most clearly in the course of the Seventies and 1980s). Indeed, numerous infectious brokers have been proposed including rickettsia (17), propionibacterium (18), streptococci or their products (19), home dust mite antigen (20), and retrovirus (21). There is increased manufacturing of immunoglobulins, together with circulating antiendothelial antibodies (25). Pro inflammatory cytokines seem to render the vascular endothelium susceptible to lysis by antibodies (27). Activated vascular endothelium expresses inflammatory antigens corresponding to intercellular adhesion molecules. Young infants have the very best fee of coronary artery aneurysm formation and sometimes current with incomplete clinical standards. Children older than age 8 years also have a better price of coronary involvement (8-10). The charges of coronary artery aneurysm based on race/ethnicity have been estimated utilizing administrative knowledge; charges were highest in Hispanics (5. Diagnosis, treatment, illness: A assertion for well being of Kawasaki management of Kawasaki from the Committee Disease, Council on Cardiovascular Disease in the Young, American professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Various mitogenic components similar to vascular endothelial development issue and platelet-derived development components are expressed throughout acute and subacute phases. Various strains of Staphylococcus and Streptococcus have been proposed because the inciting immune perturbation, with toxins performing as super antigens recruiting T lymphocytes bearingVj32 and Vj38 receptors (30). The similar investigators demonstrated immunohistochemical proof of antigens within the respiratory epithelium and macrophages that react with artificial IgA antibodies genetically engineered from these plasma cells (32). Involvement of intracranial arteries or intra parenchymal vessels inside stomach organs is extremely rare. Clinical evidence of myocarditis could also be current in the acute section, and may persist into the first three to four weeks; proper ventricular biopsies present mononuclear cell infiltration and edema inside the myocardium and conduction system and late myocyte hypertrophy and fibrosis (50,51). Inflammation persists within the walls of medium and enormous arteries as a panarteritis, with explicit predilection for the coronary arteries, and is characterized by edema, mononuclear cell infiltration, and progressive fibrosis with disruptions in the internal elastic lamina. Such harmful changes result in aneurysm formation and are most typical within the proximal segments and branching points of the coronary arteries, suggesting a job for hemodynamic stress in development of aneurysms (53). Aneurysms may be fusiform, saccular, cylindrical, or segmented (resembling beads on a string) (54,55). Erythema and edema of the arms and feet could also be accompanied by fusiform swelling of the proximal interphalangeal joints of the arms. The most dramatic extremity symptom is gangrene of fingers and toes, which occurs hardly ever in very young infants, mostly of non-Asian background (57). Clinical and spinal fluid findings of aseptic meningitis could additionally be present within the acute phase. During this time, most patients show desquamation beginning in the subungual regions and spreading to the palms and soles. In addition to the principal signs, there may be hepatomegaly, hydrops of the gallbladder (58), transient jaundice, and irregular liver function tests. In the genitourinary system, the affected person may show signs of urethritis and phimosis (in uncircumcised males) typically accompanied by dysuria and sterile pyuria. Transient and isolated peripheral nerve impairment similar to facial palsy, phrenic nerve paralysis, or sensorineural listening to loss has additionally been described (59,60). If the patient remains untreated or is handled with aspirin solely, the febrile course normally lasts from 1 to 3 weeks. The affected person might show transient anemia and leukocytosis with elevated numbers of neutrophils and bands. All scientific options are hardly ever current at the same time, so the prognosis requires sequential analysis of the patient with detailed day-by-day history of the current sickness. Elevations of liver perform tests, together with plasma gamrna-glutarnyl transpeptidase, transaminases, and bilirubin, are additionally frequent (62,64). Lumbar puncture may present findings suitable with aseptic meningitis, with a predominance of mononuclear cells, but with normal glucose and protein levels (65). Clinical Features: Cardiovascular During the acute part, sufferers could manifest indicators of myocarditis, such as sinus tachycardia out of proportion to the fever, gallop rhythm, and sometimes muffled coronary heart tones. Systolic murmurs are sometimes heard owing to elevated cardiac output and anemia, and approximately one-quarter of patients have mitral insufficiency (72). The Japanese National Kawasaki Disease surveillance data estimates the incidence of coronary aneurysms to be between 10. An aneurysm within the distal arterial phase is normally however not all the time accompanied by an aneurysm in the proximal phase of the identical artery. Aneurysms with internal diameters >8 mm or a z-score of ~10 (so-called big aneurysms) current disproportionately larger dangers of myocardial infarction as in contrast with aneurysms of smaller dimensions (75,76). Several risk scores have been formulated to predict the development of coronary artery aneurysms primarily based on scientific and laboratory information at presentation (77-81). Younger age in particular appears to be an essential predictor for worse presentation. For these sufferers, one should think about different diagnoses (see Diagnosis and Differential Diagnosis, Table 59. Rarely, the chest x-ray could present localized pulmonary infiltration or pleural effusion. Patients whose coronary aneurysms persist ~1 year after the onset of the illness might present a thin, eggshell-like calcification outlining the aneurysms. Myocardial dysfunction is associated with a larger threat of coronary artery dilation (72). Echocardiography is often repeated at 2 and 6 weeks after the onset of illness to see the extent of coronary involvement and to information therapy. For patients with giant aneurysms, we perform echocardiograms twice weekly early in the illness, then weekly through the first 45 days of illness, month-to-month until the 3rd month, and then every 3 months for the primary yr to assess for thrombosis. For long-term cardiac follow-up, echocardiography is helpful for evaluating global left ventricular perform, regional wall motion characteristics, and competency of mitral and aortic valves. Proximal segments of the best and left coronary arteries could additionally be visualized in practically all patients. Visualization of distal coronary artery segments may be technically demanding, necessitating patient sedation, use of special views (87), and careful optimization of machine settings. Standards printed by the Japan Kawasaki Disease Research Committee use an empiric definition of abnormality (89). By these requirements, a coronary artery is assessed as abnormal if (a) the inner diameter is >3 mm in children younger than 5 years of age; (b) the interior diameter is >4 mm in kids ~5 years of age; (c) if the internal diameter of a segment measures 1. Representative electrocardiogram leads in a 4-month-old girl with Kawasaki illness recorded on illness days 17 and 20. The latter tracings show marked decrease in R-wave voltage (V2-V5), indicative of acute anterior wall infarction, which was confirmed at post-mortem. Chest pain is reported a lot less incessantly in children youthful than 4 years of age. Approximately one-third of the patients are asymptomatic at the time of infarction, which regularly occurs at relaxation or throughout sleep, and infrequently during exertion (82). Fatality associated with the first episode of myocardial infarction has been reported to be 22%, with a progressively worsening mortality charges with subsequent attacks.
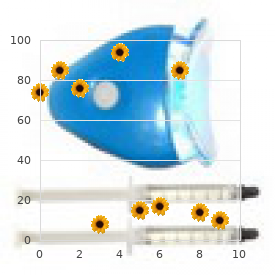
15 mg meloxicam purchase with visaThe major end point arthritis in neck and hands meloxicam 15 mg buy discount on line, time to chest closure arthritis knee exercises cycling purchase meloxicam 7.5 mg with visa, was actually extended within the therapy group. No distinction was noted within the secondary end points of surgical blood loss or use of blood products (102). The Propensity for Thrombosis in Adolescents and Children with Congenital and Acquired Heart Disease Congenital and acquired coronary heart disease put adolescents and kids at risk for thrombosis mainly as a end result of the triad of danger factors for thrombosis initially described by Virchow (131) in 1856 is usually at play. Therefore, danger factors for thrombus in adolescents and children with heart disease should be expanded to embrace: 1. Hypercoagulability: Coagulation abnormalities have been identified to include altered coagulation protein levels, decrease endogenous inhibitors of coagulation, and decreased fibrinolytic proteins among others. Such coagulopathies were first recognized in youngsters and adolescents with a Fontan circulation however more recently have been found in children through all phases of single-ventricle palliation and likewise in children with acyanotic and purchased heart disease (121,122,a hundred twenty five,126,133-138). Stasis: could happen in dilated coronary heart chambers as well as in dilated native or prosthetic outflow tracts. Turbulent flow: is a move throughout stenotic native or prosthetic coronary heart valves, stents, and/or obstructed outflow tracts with increased sheer stress that can outcome in platelet activation impartial of endothelial harm (139). Endothelial disruption: occurs from turbulent move on endothelial surfaces in addition to vessel wall endothelial damage from insertion and persistence of central lines and catheters. Endothelial injury, as discussed beforehand, exposes tissue factor and subendothelial collagenstimulating platelet aggregation and coagulation on the site of harm. Note, platelets can be activated by other mechanisms in addition to endothelial damage corresponding to from cytokines launch during irritation (139-141). Thrombosis Thrombosis in Children and Adolescents with Congenital and Acquired Heart Disease Thrombosis has long been recognized as a clinical problem to the clinician caring for adolescents and kids with congenital and acquired coronary heart disease. Much work has focused on the analysis, remedy, and prevention of thromboses in Kawasaki illness (104-107) and to a lesser extent on the thrombotic issues related to cardiac catheterization (108-111) or cardiomyopathies (112,113). For the past decade, the one ventricle population has been recognized as a particularly high-risk inhabitants for thrombosis and their doubtlessly devastating sequelae (119-128). Two retrospective research reviewed thrombotic incidence and threat factors in cardiovascular surgical populations. Deep venous thromboses related to indwelling central traces were the commonest. Wide dose ranges have been reported (17-200,Ug/kg) Lower doses are advisable 4lHiO,Ug/kg Severe bleeding proof against maximized part therapy. Interestingly, all of the above-mentioned danger components together with coagulation abnormalities, altered blood move, endothelial harm, and abnormal vascular surfaces are operative. Inflammation and bloodstream an infection: Tissue issue has been documented to become accessible by way of activated monocytes or endothelial cells when stimulated by sepsis or through cytokine production throughout irritation (140,142). In latest medical studies, sepsis was associated with increased thrombus formation especially in the presence of an indwelling central venous catheter (144-146). Consequence of Significant Thrombi in Adolescents and Children with Cyanotic Heart Disease Adolescents and youngsters with cyanotic coronary heart illness are at particular risk of devastating problems from each venous as well as arterial thrombi. Occlusion of systemic-to-pulmonary shunts or Fontan circuits are both deadly without immediate intervention. Postcatheterization arterial or venous thrombotic occlusions may make performance of additional important diagnostic and/or therapeutic cardiac catheterizations troublesome to inconceivable. The presentation of perioperative thrombi could additionally be insidious, for instance, low-grade fever and/or thrombocytopenia from platelet consumption within the thrombus. Areas notorious for difficult-to-image thrombi are Fontan baffles/conduits and right ventricular outflow tract patches/conduits, each of which are often seated anteriorly, limiting noninvasive imaging. It is unclear, nevertheless, whether or not subgroups exist where such prophylaxis may be useful. Platelet inhibition achieved in 60 min Half-life 10 h Elimination primarily through excretion biliary Dipyridamole 2-5 mg/kg divided each 6-8 h None Clopidogrel 0. Maneuvers to improve systemic blood stress thereby rising shunt flow (phenylephrine, epinephrine) Maximize oxygen supply and reduce oxygen consumption (intubation, mechanical ventilation, muscle paralysis) Fontan There has been a lot curiosity over the past 20 to 30 years in thrombosis after the Fontan operation (123,124,127,157164). The incidence of thrombotic complications after the Fontan operation has been reported to be 3% to 33% general (1. Although these critiques are an essential supply of observational information, their heterogeneous designs limit the power to draw conclusions from which apply guidelines may be generated. The following observations, nevertheless, could be made: � There appear to be two peaks in the incidence of thrombotic problems post-Fontan: early (3 to 6 months postoperatively) and late (5 to 10 years after the Fontan) (159,161,165). Identified risk factors for thrombosis embody flow stasis, ventricular dysfunction, arrhythmias, bilateral bidirectional cavopulmonary anastomoses, hypoplastic cardiac chambers with flow stasis, presence of a blind ended pulmonary artery stump, Kawashima connection, historical past of previous thrombosis, protein-losing enteropathy, extended pleural effusions, and prolonged immobilization. Occlusion or near-occlusion should be treated expeditiously with intravascular stenting, handbook shunt manipulation, or shunt revisions. Systemic thrombolytic remedy is often not used in aortopulmonary shunt occlusion since it may complicate subsequent emergent catheterization and/or surgical procedure. Partial shunt thrombosis presents with unexplained O 2 saturations lower than baseline with out one other etiology. An angiogram is often beneficial for affirmation since concomitant balloon dilation could also be useful for nonocclusive thrombus and stent placement for distortion or kinking on the insertion website. Event charges have been 38% for the composite finish point, 26% for demise, and 12% for shunt thrombosis. Investigation into alternative means of thrombosis prevention in these high-risk populations is warranted. At any stage in the single ventricle pathway, sure factors, along with these mentioned above, might put a affected person at increased danger for thrombosis including circulate stasis, ventricular dysfunction, previous thrombosis, protein-losing enteropathy, prolonged pleural effusions, arrhythmias, prolonged immobilization, and/or an irregular thrombophilia profile. Initiation of prophylactic anticoagulation remedy or increasing the magnitude There are restricted retrospective evaluations on using prophylactic anticoagulation after the Fontan operation. Transthoracic and transesophageal echocardiograms have been performed at three and 24 months post-Fontan. All thrombi have been venous, seventy two % have been detected on routine echocardiogram, and 28% had been associated with clinical signs/symptoms. Thrombi had been detected by transthoracic echo in fifty two % and by transesophageal echo in 84%. The second peak in thrombosis danger (5 to 10 years post-Fontan) warrants rigorous investigation as well. Conclusions that can be drawn from the at present available data relating to monitoring and prophylaxis of the Fontan affected person: � Since the risk for thrombotic issues may change over time, repeated scientific screening for adjustments in anatomic and hemodynamic risk elements seems indicated. Close monitoring for thrombosis with periodic transthoracic echocardiography with centered consideration to the identification of thrombi must be a half of routine of post-Fontan care. There is rising evidence that sure sufferers are "repeated clotters" and their propensity to thrombosis may warrant a better level of surveillance and possibly a higher stage of prophylaxis (128). Antiplatelet remedy for prophylactic long-term anticoagulation appears affordable after the Fontan operation. Further identification of threat elements, sufferers at explicit individual danger ("clotters"), various agents, as nicely as various management strategies are important.
|