Purchase 80 mg inderal amexSinonasal squamous cell carcinoma is often seen in immunocompetent sufferers and reveals an aggressive antral gentle tissue mass with secondary bone destruction of sinus walls and extension into multiple adjoining neck and orbital compartments blood pressure tester discount inderal 80 mg otc. It usually includes the nasal septum and turbinates and rarely includes the sphenoidal sinus pulse pressure lying down inderal 40 mg buy without a prescription. Acute inflammation of sinonasal mucus is extra widespread inside the maxillary and ethmoidal sinuses, with presence of air-fluid levels containing bubbly or frothy secretions. There could also be mucosal thickening or opacification of sinuses, but no associated perisinus gentle tissue infiltration or bone erosion should be present. Melanotic melanoma displays low T2 signal and mildly high T1 signal because of the presence of melanin, free radicals, metallic ions, and hemorrhage. Inflammation of sinuses and nasal cavity for more than 12 consecutive weeks is taken into account as continual rhinosinusitis. There is thickening of mucosal lining with or without gentle tissue opacification because of continual inflammation. The retained secretions can exhibit high T1 and low T2 signal due to chronic inspissation and increased protein content. Aggressive pyogenic sinusitis can lead to subperiosteal and postseptal abscess, cavernous sinus thrombosis, or meningitis. Air-fluid levels are widespread, with areas of mucosal thickening, and bony erosion is less common. The most dreaded acute invasive form is seen in severely immunocompromised patients, while the persistent kind is more common in diabetics. Areas of bone erosion are widespread, with infiltration of adjacent fat and soft tissues. Intraorbital and intracranial extension takes place along the perivascular or perineural spread [1] or through direct bony invasion. Fungal parts may cause low T2 sign, which can look analogous to air inside the sinuses. Intracranial extension through cribriform plate and orbital invasion is frequent when ethmoidal sinuses are involved. Involvement of the maxillary sinus results in encroachment of retroantral fat or premaxillary soft tissue. Mucormycosis is more commonly associated with acute invasive fungal sinusitis, while in more than 50% of instances with chronic invasive fungal sinusitis Aspergillus fumigatus is the wrongdoer. Importance Acute invasive fungal sinusitis is associated with a really excessive, up to 80%, mortality without appropriate medical and surgical remedy. Rapid orbital involvement, cavernous sinus thrombosis, carotid occlusion, and cerebral infarction and hemorrhage are a few of the morbid issues. Radical surgical resection and debridement with systemic antifungal therapy is the therapy of choice. Teaching factors High index of suspicion is crucial for the diagnosis of invasive fungal sinusitis. Even refined periorbital or leptomeningeal enhancement signifies extension of disease exterior the paranasal sinus and requires immediate and aggressive intervention. Specific consideration should be directed to the cavernous sinus and inside carotid artery in instances where the sphenoid sinus is concerned. Typical scientific situation Rapidly progressive fever, congestion, nasal discharge with complications and orbital ache in an immunocompromised patient is the most common clinical presentation for acute invasive fungal sinusitis. Chronic sinus pain, nasal discharge, fever, and epistaxis are extra common presenting symptoms. Punctate foci of bone demineralization and erosion are seen alongside the anterior and medial wall of the best maxillary sinus (short arrows). There is permeative destruction of the medial and posterior lateral wall of the maxillary sinus (short arrows). The intracranial extension of fungal granuloma reveals iso to mildly excessive T1 signal (arrow). Low T2 signal fungal mass at posterior proper ethmoidal (arrow) and anterior left ethmoidal air cells exhibit sign depth similar to air throughout the posterior left ethmoidal air cells. There is transforming of proper lamina papyracea with extension of invasive sinusitis into the medial right orbit (arrow). Note enhancement within the left facet of the clivus and the best side of the nasopharynx. There is presence of inflammatory tissue obstructing the right ostiomeatal complex (short arrow). Low T1 sign polypoid mucosal thickening is seen at bilateral maxillary sinuses (long arrow). High T1 signal retained secretions are seen at left maxillary sinus (short arows). High T2 signal polypoid mucosal thickening is seen at bilateral maxillary sinuses (long arrow). Enhancement of the mucosal edges of polypoid thickened maxillary sinus mucosal lining with water content is seen (long arrow). Mistaking cephaloceles for inflammatory mucosal change can have catastrophic penalties. Welldefined delicate tissue and fluid attenuation constructions may be seen in the sinuses adjacent to the bone defect and symbolize meningoceles or encephaloceles (collectively often recognized as cephaloceles). Arachnoid pits are more incessantly present in circumstances of cephaloceles than in regular individuals. Anosmia, proptosis, facial or temporal swelling, and extraocular muscle palsies may be seen, relying on the scale and the path of the tumor spread. Larger and extra vascular tumors show apparent circulate voids inside the mass, representing intratumoral vessels. The tumor is believed to arise from the lateral margin of the posterior nasal cavity, adjacent to the sphenopalatine foramen. Large tumors are dumbbell-shaped or bilobed, with one portion of the tumor bulging into the nasopharynx and the other extending towards the pterygopalatine fossa. These tumors can demonstrate extensive locoregional unfold alongside pure tissue planes. Superiorly, the mass can erode into the sphenoid sinus, cavernous sinus, sella, and middle cranial fossa. Laterally, the tumor may unfold into the pterygomaxillary and sphenopalatine fossae. Larger tumors trigger a characteristic bowing of the posterior wall of the maxillary sinus. Occasionally the mass can erode via the higher wing of the sphenoid bone, thereby exposing the dura of the center cranial fossa.
Purchase inderal 40 mg visaDespite the mechanistic variations between the two antidepressant lessons blood pressure before heart attack order inderal 40 mg, the literature has not been in a place to blood pressure medication kills cheap inderal 40 mg visa conclusively demonstrate a distinction between them by method of their capability to manage neuropathic ache. Serotonin�norepinephrine reuptake inhibitors Duloxetine and milnacipran are another class of antidepressant medication used in the treatment of neuropathic ache. Central immune signaling the neuronal hypothesis of neuropathic ache has been complemented within the last two decades by heightened appreciation of the role that central immune signaling, from cells corresponding to glia and their pro-inflammatory signaling molecules, these generally investigated being cytokines and chemokines, have in neuropathic ache. Both astrocytes and microglia in the spinal cord are activated (defined immunohistochemically by elevated expression of activation markers) in response to inflammation and damage of peripheral tissues, peripheral nerves, spinal nerves, and spinal twine. Enhanced ache related to each persistent animal ache model examined to date is blocked by disruption of glial activation and spinal twine proinflammatory cytokine actions. It is with this nice promise that a lot drug improvement has progressed on this revolutionary space. However, to date solely two brokers opportunistically developed to broadly goal central immune signaling, ibudilast and propentofylline, have ventured into scientific trials, with combined results. Other agents that selectively goal particular pro-inflammatory/pronociceptive cytokines or chemokines are also within the pipeline. It is crucial to note that no new chemical entity to target this mechanism has ventured this far. A nice variety of limitations, including scientific, educational, and "cultural" have to be overcome earlier than the non-neuronal origins and propagators of neuropathic ache are clinically exploited in the remedy of neuropathic ache. However, the medical demand for more practical neuropathic ache administration and treatment suggests all classes of pharmacological agents that meet the preclinical efficacy and security standards deserve medical evaluation in appropriately designed and executed studies. These last two factors bear critical consideration from scientific and regulatory vantages. Therefore, new progressive governance and steering for the development of those brokers is required (Table 29. Biomarkers for neuropathic ache Neuropathic pain is troublesome to treat because of the continued limited understanding of its complicated pathophysiology, as outlined above. Current remedy options proceed to provide solely symptomatic reduction leading to unmet medical want. Chronic pain is currently assessed by clinicians with using self-reports (such because the visual analog rating report) as no validated biomarker for neuropathic ache has but been developed. The use of these subjective reports could be ineffective in scientific trials for new analgesics improvement as only profound variations could be detected [14]. There is an pressing need for an goal, credible, and validated check for persistent (neuropathic) pain. Biomarkers also can enrich clinical trials by selecting sufferers extra more doubtless to respond to a new remedy, allowing for personalization (doses or frequency or both) of the remedies, aid early drug growth by growing effectivity, and speed up determination making in drug target choice and improvement [16]. To date, no accredited biomarker is presently being utilized in qualifying continual pain due to the difficulties in finding biomarkers as a outcome of the inaccessibility of the central anatomical compartments and the dynamic nature of persistent pain. However, many researchers are currently on the lookout for potential targets and a few are wanting promising. The trend for genetic polymorphism discovery will proceed to increase as new targets are being identified and along with the interplay of environmental factors, will greatly help the prognosis and intervention for continual (neuropathic) ache sufferers. Immune signaling protein targets In the previous 20 years proof has developed suggesting central immune signaling performs an necessary position in the initiation and establishment of continual pain. Mediators of the immune cells corresponding to pro-inflammatory cytokines and chemokines (interleukin-8 and monocyte chemotactic protein-1) have been discovered to correlate with the severity of fibromyalgia [18] and chronic pelvic ache syndrome [19]. Quantification of peripheral blood pro-inflammatory mediators is slowly rising as a possible candidate for pain markers. These all contribute to the identification of potential biomarkers for persistent (neuropathic) ache. A single biomarker alone is unlikely to capture the complexity and multidimensional nature of persistent ache because it entails many methods. Instead of replacing subjective self-reports, biomarkers would work synergistically with existing habits tests, scientific historical past, and genetic make-up in allowing clinicians to higher characterize and diagnose persistent pain patients and monitor therapeutic intervention. Genetic polymorphisms Genetic markers can be considered as biomarkers for neuropathic pain, as latest reviews have discovered some neuropathic ache to present substantial heritability. Emerging proof has additionally been found to present that genes encoding for pro-inflammatory cytokines (interleukin Non-pharmacological interventions for neuropathic pain Current pharmacological interventions for neuropathic ache have massive numbers wanted to deal with and are sometimes ineffective for the long-term management of neuropathic pain. Consequently, extra healthcare 348 Chapter 29: the lengthy run: new concepts and potential therapies practitioners are encouraging sufferers with neuropathic ache to search non-pharmacological interventions to manage their pain. Non-pharmacological interventions are considered to be cost-effective pain interventions because of their relatively low value and their potential to reduce antagonistic occasions due to drug�drug interactions, probably decreasing healthcare utilization costs by way of decreased hospital admissions. Furthermore, although non-pharmacological therapies are nonspecific in their mechanistic nature, these therapies have proven to be as, or much more efficient, in some individuals in contrast with focused pharmacological therapy. Given the complicated, multimodal pathology of neuropathic pain outlined above, therapy choices with broad strokes like this are extremely beneficial. Consequently, just like pharmacological prescribing for neuropathic ache, non-pharmacological therapies must be co-prescribed with other nonpharmacological therapies, or even as adjunct therapies to frequent pharmacological interventions so as to target the multiple methods concerned in neuropathic pain. Below is a brief abstract of a number of the non-pharmacological therapies used for continual neuropathic pain administration and tabulated proof supporting their continued use. Brain stimulation Several types of brain stimulation are available and shall be outlined below. Before mind stimulation could be carried out in medical practice for neuropathic ache, further trials are required to higher decide whether non-invasive cortical stimulation methods can induce long-lasting effects. Stimulating particular factors on the physique, with skinny stable needles, can appropriate imbalances within the flow of qi via channels generally known as meridians. Cranial electrotherapy stimulation is being thought of a safer various to drug remedies for so much of circumstances corresponding to insomnia, despair, drug addiction, complications, and even consideration deficit hyperactivity dysfunction. Heat remedy Heat helps chill out muscle tissue and improve tissue temperature, leading to blood vessel dilation, resulting in improved blood circulation and supply of oxygen and nutrients, as nicely as removing of carbon dioxide and metabolic waste from the injured tissue. Pain signals are inhibited, on the dermatomal stage, by an electrical present earlier than they reach the mind. Spinal twine stimulation is recommended for sufferers with pain refractory to typical pharmacological therapies. Illusions Illusions are distortions of sensory notion, doubtlessly revealing how the mind usually organizes and interprets sensory data. Mirror field remedy involves the affected person viewing their practical limb in lieu of their missing, injured, or paralyzed limb, thus tricking the mind into believing that their lacking, injured, or paralyzed limb is moving freely with no restrictions. Exercise Frequent and regular exercise boosts the immune system, improves psychological well being, helps prevent depression, helps to promote and maintain optimistic vanity, reduces cortisol, improves sleep, and produces endogenous opioids, thus doubtlessly decreasing ache and strengthening muscles surrounding the damage site, thus reducing stress off the injured area. It has been demonstrated that all sufferers who devour therapeutics are topic to the placebo effect. Furthermore, the mechanism of motion of quite a few non-pharmacological remedies for persistent neuropathic ache is believed to be mediated by way of the placebo impact. Consequently, clinicians could possibly tailor their angle in direction of sufferers to potentiate the placebo effect and thus improve their neuropathic ache therapy outcomes. The inclusion of placebos (inactive substances) in randomized placebo-controlled scientific trials, in this occasion for analgesics, typically hinders the effect of the investigational remedy and thus inclusion of placebos is usually dreaded by clinical researchers/pharmaceutical firms. Massage Massage entails working superficial and deeper layers of both muscle and connective tissue using various techniques, corresponding to strain, tension, or vibration. Massage remedy can improve bodily operate, speed up the healing process and promote relaxation and well-being by improving oxygen and nutrient circulation to the injured tissues, relieving rigidity and ache, rising flexibility and mobility, and clearing waste from the harm web site.
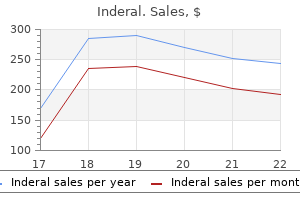
| Comparative prices of Inderal | | # | Retailer | Average price | | 1 | Family Dollar | 985 | | 2 | Ruddick Corp. | 217 | | 3 | Gap | 379 | | 4 | Williams-Sonoma | 879 | | 5 | Toys "R" Us | 362 | | 6 | YUM! Brands | 121 |
Buy 80 mg inderal free shippingI would correlate these findings with the scientific historical past and evaluation previous imaging arrhythmia with normal ekg 40 mg inderal visa. This situation can be sometimes related to brief fourth and fifth metacarpals arrhythmia statistics inderal 80 mg cheap fast delivery, so asking to see a earlier hand radiograph would additionally demonstrate your wider data. There are multiple, well-defined excessive attenuation lesions predominantly located at the grey�white matter junction. The most typical primary tumours to metastasise to the brain are lung and breast carcinoma; nevertheless, haemorrhage is also related to melanoma, renal and thyroid primaries. To take this additional, I would evaluation any previous imaging for proof of a major malignancy. In this case, multiple well-defined haemorrhagic lesions at the grey�white matter junction are strongly suggestive of metastatic disease. They are normally discovered on the grey�white matter junction due to the small calibre of vessels on this space. Pearls Multiple enhancing lesions, located on the grey�white matter junction, with a disproportionately great amount of surrounding oedema, are suggestive of metastatic illness. Lung, breast, melanoma and renal primaries are the most typical causes of mind metastases. There is a well-defined intra-axial mass throughout the left frontal lobe, which demonstrates excessive T2 signal. There is a less well-defined area of elevated T2 sign inside the white matter surrounding this lesion, consistent with oedema. If there was an extended historical past of symptoms, I would additionally contemplate a major mind malignancy or a big cystic metastasis. To take this further, I wish to see contrast-enhanced T1 and diffusion-weighted images to aid further characterisation. However, the presence of restricted diffusion is suggestive of lymphoma, but not a glioma or metastasis. Pearls Key options to mention with all mind lots are their location, T2 signal intensity, enhancement sample and associated oedema. There is an intensive abnormality within the distal spinal twine and conus that extends over a length of a minimum of five vertebral body heights. It contains focal areas of high and low T2 sign, which may symbolize cystic change and haemorrhage, however correlation with T1 images is required. Discussion Intramedullary spinal lesions lie within the substance of the spinal cord. Ependymomas are extra common in adults, whereas astrocytomas are the most common spinal tumour in kids. Bony remodelling is a useful signal that can be utilized to assist distinguish between an ependymoma and an astrocytoma. Ependymomas are slow-growing tumours with an insidious onset of symptoms together with again pain, sensory loss, and bowel and bladder dysfunction. This sluggish fee of growth is related to bony remodelling, similar to pedicle erosion, laminar thinning and posterior vertebral body scalloping, all of which result in widening of the spinal canal. These conditions have classical multisystem imaging features, so are seen extra usually in the examination than in actual life. They are associated with a disproportionately giant space of cord oedema with respect to the scale of the lesion. Most intramedullary plenty are both ependymomas (more common in adults than children) or astrocytomas (more frequent in kids than in adults). There is a focal mass lesion within the spinal canal at the level of the conus medullaris. The lesion is separate from the twine, which it displaces anterolaterally to the proper. When compared to the spinal cord, the lesion demonstrates reasonably high T1 sign, and on T2 sequences is isointense. As this is an adult patient, the most likely analysis is a spinal metastasis, maybe secondary to melanoma. The differential diagnoses for an intradural extramedullary lesion also embody nerve sheath tumours and meningioma. Discussion Intradural extramedullary masses are positioned outdoors of the spinal wire but inside the dural sac. Neurofibromatosis is a vital multisystem disorder in the context of the exams. If you think you studied this condition, knowledge of the outlined diagnostic standards and other related manifestations ought to be used to formulate your management plan for further imaging. It may not be possible to distinguish reliably between a neurofibroma and schwannoma as they share comparable imaging traits. This look occurs when the tumour has each an extradural and an intradural component and is narrowed within the middle because it passes through the neural foramen. These options will allow you to distinguish a nerve sheath tumour from metastases and meningiomas. This case checks your capability to combine two diagnostic lists � one for the intradural extramedullary mass and the opposite for a lesion with high T1 signal. This scenario is relatively frequent in the viva setting and tests your ability to course of data sensibly when confronted with a number of imaging options. Haemorrhage and fat (lipoma/dermoid) can have a excessive T1 signal but neither improve. Melanin produces a excessive T1 signal and melanoma metastases can improve, due to this fact a melanoma metastasis is a wise proposition in this case. Substances with a excessive sign on T1-weighted imaging include subacute haemorrhage (methaemoglobin), fat, protein, melanin and distinction. There is extensive, intermediate T1 and T2 signal materials within the spinal canal. This surrounds the cauda equina at the level of L3 and L4, and extends superiorly in the posterior facet of the spinal canal to at least the T10 stage and beyond the higher restrict of the offered photographs. On the axial image, the lesion is positioned exterior the thecal sac, in preserving with an extradural location. Discussion Intraspinal plenty could also be extradural (as in this case), intradural extramedullary (Case 43) or intramedullary (Case 42). It is significant to localise accurately a spinal mass to considered one of these three compartments early in your description of a case, as it will lead you to the proper record of differential diagnoses. In every day follow, there are several conditions that require urgent action when identified. Good examples of these embrace a rigidity pneumothorax, leaking belly aortic aneurysm, suspected non-accidental damage and spinal cord compression.
Generic 80 mg inderal fast deliveryOther patterns of unfold include involvement of the infratemporal fossa through the medial orbital wall and involvement of the middle cranial fossa from extension via the superior orbital fissure and sphenoid wing arteria subclavia inderal 80 mg discount mastercard. Esthesioneuroblastoma(Olfactory Neuroblastoma) Identification of meningiomas with atypical options is necessary blood pressure medication options inderal 40 mg discount amex, with implications for treatment and long-term responsiveness to neoadjuvant chemotherapy and radiation therapy. Studies have demonstrated that atypical meningiomas could be distinguished on the basis of their sign depth on diffusionweighted imaging and fractional anisotropy maps. Apparent diffusion coefficient maps additionally could additionally be helpful as a result of meningiomas with atypical options usually are isointense or barely hypointense, in distinction to low-grade or "typical" meningiomas (which predominantly are hyperintense). SinonasalEpithelialMalignancy Another lesion within the differential of anterior fossa mass lesions is the esthesioneuroblastoma, which tends to occur within the second and sixth many years. This malignancy sometimes arises along the olfactory groove or the higher nasal cavity because of the neuroendocrine derivation of the basal layer of the olfactory mucosa. The basic imaging appearance is a bilobed, dumbbell-shaped mass with central "waisting" at the cribriform plate. These mass lesions usually present comparatively late in the course of the malignancy and usually are massive with regional transforming that seems to be chronic. When seen in their early type, this lesion can appear as a small, off midline, polypoid mass of the superior nasal cavity. The presence of high T2-signal marginal cysts has been described as a diagnostic indicator of this malignancy; nonetheless, this traditional manifestation is uncommon. Medial orbital wall invasion or intracranial extension into the anterior cranial fossa is often seen at the time of diagnostic imaging. MetastaticDisease Sinonasal epithelial malignancy is a vital diagnostic consideration. These lesions reveal a transcompartmental morphologic sample, reflecting the primary pattern of tumor development via direct extension and infiltration of the intracranial contents from the sinuses, classically from the ethmoid air cells. In the pattern case, infiltration that seems to be aggressive is famous by way of the ground of the anterior cranial fossa One of the most typical etiologies for intraparenchymal cerebral mass lesions is hematogenous dissemination of metastatic disease. Of the recognized biopsy-proven neoplasms, lung cancer leads the listing (as excessive as 80% in some series), adopted by other widespread main neoplasms including breast cancer, melanoma, and colorectal most cancers. The introduced case is a biopsy-proven metastatic colon cancer focus to the anterior cranial fossa. Note that a key level of distinction from the aforementioned transcompartmental lesions is the intraaxial localization of the lesion throughout the parenchyma of the frontal cortex. The mass appears transcompartmental, extending from the paranasal sinuses through the ground of the anterior cranial fossa and bilateral medial orbital walls. This lesion is radiographically indistinguishable from a sinonasal epithelial carcinoma, with the analysis hinging on pathologic sampling. These neoplasms have the propensity to be fairly massive on the time of presentation, with involvement of the nasal cavity and paranasal sinuses, and so they typically extend into the anterior cranial fossa directly by way of the cribriform plate and ethmoid roof. Anosmia can happen from invasion of the olfactory bulb or nerves or from blockage of air move to the upper nasal cavity. Infiltration of the cranium base foramina also can outcome in cranial nerve V nerve deficits, with specific extension into the middle cranial fossa and involvement of the foramen ovale and/or foramen rotundum. Meningiomas uncommonly can bear malignant degeneration into meningosarcoma or atypical meningiomas. Symptoms can range from complications and hearing loss or vestibular dysfunction to facial paralysis or diplopia. Most benign processes are related to the presence of petrous apex pneumatization, a traditional physiologic variant that happens in as a lot as 30% of the population. The neoplastic processes include both benign entities, such as meningiomas and schwannomas of the facial, trigeminal, or abducens nerves and their branches, and malignant processes, consisting of major neoplasms. Asymmetric pneumatization of the petrous apices is commonly observed but may be misconstrued as a pathologic course of. The pneumatized apex will be hypointense on T1-weighted imaging, resulting in asymmetric T1-hyperintense fat sign within the bone marrow of the contralateral nonpneumatized petrous apex. The presence of fluid sign throughout the in any other case normally developed petrous apex cells and the absence of expansion or harmful modifications in the adjacent bone suggest the analysis of trapped fluid within the petrous apex. Some centers continue to monitor these lesions with imaging to ensure stability and to exclude more aggressive entities. However, the presence of an intermediate or hyperintense T1 signal suggests either proteinaceous fluid or a growing cholesterol granuloma, in which case correlation with clinical historical past and imaging follow-up is necessary in all cases. Cholesterol granulomas (or cholesterol cysts) are expansile, T1- and T2-hyperintense lesions of the petrous apex that will reveal peripheral enhancement and are thought to characterize inflammatory granulation tissue, which develops in response to ldl cholesterol crystals within the isolated petrous apex cells. Mucoceles of the petrous apex are much more rare than cholesteatomas in this location. Additional imaging features include enlargement and easy scalloping of the adjoining bony margins and absence of enhancement. The presence of trabecular breakdown in opacified petrous air cells with concurrent mastoid air cell opacification and rimlike enhancement of the fluid-filled cells is extremely suspicious for petrous apicitis. Advanced circumstances of petrous apicitis may show thickening and enhancement of the adjoining meninges, venous sinus thrombosis, fistulization into the labyrinth, petrous carotid pseudoaneurysm, and findings of cranium base osteomyelitis. The presence of osseous destruction and septal erosion ought to elevate concern for one of many neoplastic processes that are inclined to contain the petrous apex, similar to a chordoma, chondrosarcoma, or those that can come up in any osseous structure, similar to plasmacytoma or metastatic disease. In a child, histiocytosis and varied sarcomas also can come up in or contain the petrous apex. Observation of fats sign intensity within the petrous apex, just like that of orbital fat and the absence of enhancement or damaging adjustments, suggests this analysis, which could be confirmed with fat-saturation strategies. In children, the marrow might not have transformed to fats, however the lack of bony growth or erosion and stability over time can suggest the diagnosis. Some persons think about mucoceles to be a part of a spectrum with cholesterol granulomas (cysts) quite than a distinct entity. Peripheral enhancement in the applicable clinical setting should recommend this analysis; nevertheless, aggressive neoplasms may have a similar radiologic appearance. Although chordomas are inclined to come up within the midline (originating from notochord remnants) and chondroid tumors normally emanate from the petrooccipital synchondrosis, the differentiation between these two entities usually is difficult on imaging. However, the presence of chondroid matrix and an off-midline locale is extra suggestive of a chondroid neoplasm. The mixture of imaging findings with clinical indicators and symptoms ends in an accurate analysis in most cases. On the other hand, care must be taken in diagnosing benign findings, such as fluid or uneven bone marrow, to avoid aggressive or incorrect management. Although ldl cholesterol granulomas and cholesteatomas are benign lesions, they may find yourself in listening to loss and fistulous communications. Neoplasms and aneurysms have to be differentiated from different entities affecting the petrous apex, as a outcome of they may lead to devastating penalties if incorrectly managed. Some of those entities have distinguishing characteristics, whereas others share overlapping imaging appearances. They are composed of stratified squamous epithelium and exfoliated keratinous materials.
Generic inderal 40 mg free shippingTetrodotoxin-resistant sodium channels of dorsal root ganglion neurons are readily activated in diabetic rats blood pressure 40 over 30 40 mg inderal buy with visa. Acute and remitting painful diabetic polyneuropathy: a comparison of peripheral nerve fibre pathology arterial blood gas interpretation 40 mg inderal generic mastercard. Corneal confocal microscopy: a non-invasive surrogate of nerve fibre damage and restore in diabetic sufferers. Axonal transport of substance P-like immunoreactivity in gangliosidetreated diabetic rats. The increased trafficking of the calcium channel subunit alpha2delta-1 to presynaptic terminals in neuropathic ache is inhibited by the alpha2delta ligand pregabalin. Possible position of spleen-derived factors, vanilloid receptors and calcitonin gene-related peptide in 115 Section 3: the Specific Condition: Peripheral Neuropathic Pain diabetes induced hyperalgesia in mice. Mitogenactivated protein kinase p38 mediates lowered nerve conduction velocity in experimental diabetic neuropathy: interactions with aldose reductase. Rapid synaptic reworking in the grownup somatosensory cortex following peripheral nerve harm and its affiliation with neuropathic ache. Diabetic peripheral neuropathy: amelioration of pain with transcutaneous electrostimulation. Acupuncture for the remedy of persistent painful peripheral diabetic neuropathy: a long-term examine. Relief of painful diabetic peripheral neuropathy with pregabalin: a randomized, placebo-controlled trial. Pregabalin for the remedy of painful diabetic peripheral neuropathy: a double-blind, placebo-controlled trial. Sodium valproate in the administration of painful neuropathy in sort 2 diabetes � a randomized placebo managed study. Sodium valproate for painful diabetic neuropathy: a randomized double-blind placebo-controlled examine. Efficacy of pregabalin for peripheral neuropathic pain: results of an 8-week, flexible-dose, double-blind, placebo-controlled study conducted in China. Efficacy and security of pregabalin for treating neuropathic pain related to diabetic peripheral neuropathy: a 14 week, randomized, double-blind, 116 Chapter 9: Diabetic and different peripheral neuropathies placebo-controlled trial. Amitriptyline relieves diabetic neuropathy ache in sufferers with normal or depressed mood. A double-blind, randomized multicenter trial evaluating duloxetine with placebo in the administration of diabetic peripheral neuropathic pain. Duloxetine for sufferers with diabetic peripheral neuropathic pain: a 6-month open-label security examine. Mechanisms of neuropathic ache and their implications for the design of scientific trials. A comparative analysis of amitriptyline and duloxetine in painful diabetic neuropathy: a randomized, double-blind, crossover medical trial. Superiority of duloxetine to placebo in improving diabetic neuropathic ache: outcomes of a randomized managed trial in Japan. Advances in neuropathic ache: analysis, mechanisms, and remedy recommendations. A comparison of amitriptyline and nortriptyline in neuropathic pain due to peripheral neuropathy. An openlabel, non-randomized comparison of venlafaxine and gabapentin as monotherapy or adjuvant remedy in the administration of neuropathic ache in patients with peripheral neuropathy. Venlafaxine extendedrelease in sufferers older than 80 years with depressive syndrome. Oxcarbazepine in painful diabetic neuropathy: a randomized, placebo-controlled examine. Clinical review: use of antiepileptic drugs in the therapy of persistent painful diabetic neuropathy. Effects of topiramate use on body composition and resting metabolic price in migraine patients. Efficacy and security of mexiletine in the treatment of painful diabetic neuropathy. Double-blind randomized trial of tramadol for the remedy of the pain of diabetic neuropathy. Observations on small blood vessels of pores and skin within the regular and in diabetic patients. Controlled-release oxycodone relieves neuropathic ache: a randomized controlled trial in painful diabetic neuropathy. Dextromethorphan and memantine in painful diabetic neuropathy and postherpetic neuralgia: efficacy and doseresponse trials. Double-blind, placebo-controlled study of the appliance of capsaicin cream in chronic distal painful polyneuropathy. Treatment of persistent painful diabetic neuropathy with isosorbide dinitrate spray: a double-blind placebo-controlled cross-over research. Lidocaine patch 5% with systemic analgesics similar to gabapentin: a rational polypharmacy method for the remedy of persistent ache. Oromucosal delta9tetrahydrocannabinol/ cannabidiol for neuropathic pain related to multiple sclerosis: an uncontrolled, open-label, 2year extension trial. Randomized placebo-controlled double-blind medical trial of cannabis-based medicinal product (Sativex) in painful diabetic neuropathy: despair is a significant confounding issue. An openlabel comparability of nabilone and gabapentin as adjuvant therapy or monotherapy in the management of neuropathic pain in sufferers with peripheral neuropathy. Practice Advisory: utility of surgical decompression for therapy of diabetic neuropathy: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Gabapentin within the therapy of painful diabetic neuropathy: a placebo managed, double blind, crossover trial. A randomized, placebo-controlled examine of oxcarbazepine in painful diabetic neuropathy. Endogenous monoamine analgesic techniques: amitriptyline in painful diabetic neuropathy. Randomized research of tramadol/acetaminophen versus placebo in painful diabetic peripheral neuropathy. Tramadol relieves ache and allodynia in polyneuropathy: a randomised, double managed trial. Watson I want I may counsel one thing for the after pains which generally are so severe as to make the patient weary of existence. William Bowman 1867 [1] A kindly understanding physician who will keep in touch together with his sufferers with intractable postherpetic neuralgia even for a very very lengthy time is extremely valuable therapeutically. Edgar Hope-Simpson 1990 [2] the efficient doctor is he who amuses his patients whereas nature results a cure. The philosophical dictionary, Voltaire (1694�1778) Introduction the primary two of the above quotations mirror the dangerous information, i. Post-herpetic neuralgia may be defined arbitrarily in several ways and for different functions.
Syndromes - Bufferin
- Arthritis
- Increased frequency of urination
- Phototherapy may be given alone or after you take a drug that makes the skin sensitive to light.
- Weight loss
- Speech and hand skill problems are mild
- Males and females 51 to 70: 2.0* g/day
- Abnormal heartbeat
- Nervousness
Generic inderal 80 mg without a prescriptionKinin B(1) and B(2) receptors contribute to orofacial heat hyperalgesia induced by infraorbital nerve constriction harm in mice and rats blood pressure norms purchase 80 mg inderal free shipping. Chemical mediators enhance the excitability of unmyelinated sensory axons in regular and injured peripheral nerve of the rat hypertension follow up 80 mg inderal purchase amex. P2X4 receptors induced in spinal microglia gate tactile allodynia after nerve injury. Disruption of the P2X7 purinoceptor gene abolishes persistent inflammatory and neuropathic ache. Genetically determined P2X7 receptor pore formation regulates variability in continual ache sensitivity. Nerve injury-activated microglia engulf myelinated axons in a P2Y12 signaling-dependent manner in the dorsal horn. P2Y12 receptors in spinal microglia are required for neuropathic ache after peripheral nerve damage. Prostaglandin E2 contributes to the synthesis of brain-derived neurotrophic factor in primary sensory neuron in ganglion explant cultures and in a neuropathic pain model. Role of prostaglandin E2 in the synthesis of the pro-inflammatory cytokine interleukin-6 in major sensory neurons: an in vivo and in vitro examine. Role of cysteinyl leukotrienes in nociceptive and inflammatory conditions in experimental animals. Leukotriene synthases and the receptors induced by peripheral nerve damage in the spinal wire contribute to the era of neuropathic ache. Activation of peripheral and spinal histamine H3 receptors inhibits formalin-induced irritation and nociception, respectively. The effect of systemically administered recombinant human nerve progress factor in healthy human topics. Antibodies to nerve growth issue reverse established tactile allodynia in rodent fashions of neuropathic ache with out tolerance. Role of mast cell activation in inducing microglial cells to launch neurotrophin. Tumor necrosis factor- will increase brain-derived neurotrophic issue expression in trigeminal ganglion neurons in an activity-dependent method. Effects of glial cell line-derived neurotrophic factor intrathecal injection on spinal dorsal horn glial fibrillary acidic protein expression in a rat model of neuropathic ache. Peripheral nerve harm alters blood�spinal wire barrier functional and molecular integrity through a selective inflammatory pathway. Cytokine mechanisms of central sensitization: distinct and overlapping role of interleukin1beta, interleukin-6, and tumor necrosis factor-alpha in regulating synaptic and neuronal activity within the superficial spinal wire. The function of proinflammatory cytokines within the era and upkeep of joint pain. Dynamic regulation of spinal pro-inflammatory cytokine release in the rat in vivo following peripheral nerve harm. Endogenous interleukin-6 contributes to hypersensitivity to cutaneous stimuli and adjustments in neuropeptides related to persistent nerve constriction in mice. The crucial position of invading peripheral macrophagederived interleukin-6 in vincristine-induced mechanical allodynia in mice. Efficacy of epidural administration of antiinterleukin-6 receptor antibody onto spinal nerve for treatment of sciatica. T cell infiltration after continual constriction damage of mouse sciatic nerve is related to interleukin-17 expression. Interleukin-17 contributes to neuroinflammation and neuropathic ache following peripheral nerve damage in mice. Interleukin-18-mediated microglia/astrocyte interplay within the spinal cord enhances 88 Chapter 7: Pathophysiology of neuropathic pain: inflammatory mediators neuropathic pain processing after nerve harm. Enduring reversal of neuropathic pain by a single intrathecal injection of adenosine 2A receptor agonists: a novel therapy for neuropathic pain. Transforming progress factor-beta1 impairs neuropathic pain via pleiotropic results. Chemokines, neuronal-glial interactions, and central processing of neuropathic ache. Excitatory monocyte chemoattractant protein-1 signaling is up-regulated in sensory neurons after continual compression of the dorsal root ganglion. Enhanced manufacturing of monocyte chemoattractant protein-1 within the dorsal root ganglia in a rat mannequin of neuropathic ache: possible involvement in the growth of neuropathic pain. Evidence that exogenous and endogenous fractalkine can induce spinal nociceptive facilitation in rats. The private and economic impacts of persistent pain are significant, as roughly half of victims are unable to work full-time and/or participate totally in the activities of every day life. Although there are a selection of current treatments obtainable for inflammatory ache, prescribed drugs for continual neuropathic pain are very often inadequate. Work described on this chapter investigates the potential role in neuropathic pain of a class of neuronal receptors previously thought to only reside on immune and glial cells. Investigations into neuropathic pain mechanisms often utilize the rationale that the onset of spontaneous exercise in neurons following peripheral nerve injury may set off irregular ache habits in rodents (perhaps better outlined in animals as hyperalgesia) and neuropathic pain in people [1]. It may then follow that the neuropathic pain state relies on persistent alterations within the physiology (spontaneous and/or ectopic discharge) of both nociceptive and non-nociceptive sensory neurons [2�4]. Many potential mediators and pathways have been examined as potential contributors to persistent neuropathic pain. Toll-like receptors the Toll-like receptor household of receptors is usually utilized by the innate immune system to sense the invasion of microorganisms by their capacity to acknowledge specific patterns of microbial parts. Given their variety, this household of receptors is proven to be current on a quantity of Neuropathic Pain, ed. This includes B cells, mast cells, natural killer cells, regulatory T cells, macrophages, monocytes, dendritic cells, neutrophils, and basophils [15]. These stimulated cells might then turn out to be the source of a number of native or distant responses, together with the increased excitability of nociceptive neurons and/or release of inflammatory cytokines, neuropeptides, or neurotransmitters. These released factors may be of nice relevance for a number of chronic inflammatory illnesses all through the body [25]. The third option of oxidation of the cysteines to sulfonates apparently abrogates each activities. Epileptic seizure situations are routinely characterised as a neurocentric illness due in massive part to the abnormally excessive or synchronous neuronal activity in the brain [48]. Recent advances suggest that the management of abnormal 93 Section 2: the Condition of Neuropathic Pain neuronal exercise could also be altered by refined adjustments in the setting including the release of molecules recognized to management neuronal function and synaptic transmission. Given recent discoveries that glial cells can modulate neuronal operate by encapsulating the neuronal synapse and maintaining neurotransmitter stability, potential sources of these neuropathological (or pro-inflammatory) molecules may include astrocytes and microglial cells [49,50]. For instance, febrile seizures in 3�5% of kids are considered to be a threat factor for temporal lobe epilepsy [51,52]. Evidence for increased synthesis of inflammatory mediators within the mind during epileptogenesis was corroborated in a quantity of studies using microarray analysis of transcripts of varied classes of genes [53,54]. The degree to which these findings prolong to treatment within the clinic remains to be seen [61]. These changes embrace speedy alterations within the properties of ion channels expressed by these neurons, as properly as longer-term modifications ensuing from new gene transcription.
Generic 40 mg inderal with mastercardIf the affected person is well blood pressure chart by age canada effective inderal 80 mg, this would most likely be because of blood pressure ranges low normal high 80 mg inderal with mastercard a earlier episode of Varicella zoster virus pneumonia. To take this further, I would review any earlier imaging and correlate the findings with the scientific historical past, in search of previous admissions for pneumonia related to chickenpox an infection. If that is an incidental discovering in an asymptomatic patient, it would not require follow-up. Discussion For most classical chest radiology viva instances, the lists of potential differential diagnoses may be long, and that is true for multiple calcified lung nodules. In the exam setting, the important thing to most chest instances is to establish the principle abnormality, outline the distribution and look for any related findings. These components ought to help you to refine your lengthy differential record to a more sensible brief listing of potential diagnoses. The capacity to do that is the key to both a successful viva exam and the ability of an excellent radiologist. In your day by day work, the lengthy list would even be of no practical value to a clinician. The finding of a number of small, calcified lung nodules is similar in both of those circumstances. Calcified lung metastases are generally secondary to sarcoma, mucinous tumours of the colon or breast, papillary thyroid carcinoma, ovarian cystadenocarcinoma and testicular tumours. Pearls To slim the list of differential diagnoses, critically evaluate whether or not there is/are: any calcified mediastinal nodes or higher lobe fibrosis (histoplasmosis/silicosis), an enlarged coronary heart (mitral stenosis), bone abnormalities (current/previous sarcoma) or a superior mediastinal mass (thyroid cancer). It is commonly useful to subdivide differential diagnoses primarily based on patient well-being, as this demonstrates information and insight: "If the affected person is clinically properly, I would consider. There is consolidation adjacent to the cavity, more pronounced inferiorly and laterally. There is a further smaller mass inside the right upper zone with a well-defined irregular define. This lesion may also contain a small cavity in its medial aspect however is predominantly strong. There is a generalised coarsening of the interstitial lung markings in the the rest of the lungs. The two massive cavitating lesions are again seen, mendacity in the posterior segments of each higher lobes. Therefore, primarily based on the radiological findings alone, the patient must be cared for in isolation. I would urgently inform the on-call chest physician and prepare for admission for isolation and antimicrobial remedy. Discussion the differential for a big cavitating lung mass accommodates the conditions seen in the mnemonic for multiple pulmonary nodules (see Case 4). The appearance is of centrilobular nodularity connecting to branching linear structures. These must be committed to memory as these instances are sometimes used as "starter" movies within the examination viva. Those that have a tendency to cavitate embody squamous cell carcinoma (nasopharyngeal, oesophageal and cervical), adenocarcinoma from the colon, melanoma and infrequently sarcoma. There is a lobulated right-sided mediastinal mass, which varieties a wide angle with the adjoining lung parenchyma. There are several well-defined ovoid opacities projected over the peripheral proper lung. Discussion the boundaries of the anterior mediastinum are the sternum anteriorly, pleura laterally and the anterior side of the trachea and posterior margin of the guts posteriorly. The anterior mediastinum contains lymph nodes, the thymus, the guts and the ascending aorta. An enlarged retrosternal thyroid gland can lie in the superior a part of the anterior mediastinum, and might be steady with the neck. For instance, if the ascending aorta is effaced, the mass should lie throughout the anterior mediastinum. A tumour of germ cell origin (teratoma) typically accommodates fat, calcifications and enhancing septations. Germ cell tumours are extra prevalent in younger folks, while thymic tumours affect older adults. Pearls A mediastinal mass types an obtuse angle with the adjoining lung parenchyma. Look for effacement of heart borders and ascending aorta to affirm an anterior location. Mention the visibility of hilar vessels by way of the mass (hilum overlay sign) indicating no center mediastinal component. Consider an enlarged thyroid if the mass lies superiorly and shows contiguity with the neck. The mass invades the left aspect of the mediastinum and is seen on these photographs to encase the aortic arch, descending aorta and the left pulmonary vein. The most probably cause is a thymic tumour, mesothelioma or adenocarcinoma metastases. To take this additional, I would review this scan on lung and bone windows to search for any proof of lung nodules or skeletal lesions to indicate metastases. The presence of circumferential pleural thickening, pleural thickening larger than 1 cm in depth, widespread pleural nodularity and involvement of the mediastinal pleura are all features associated with malignancy. However, definitive differentiation of benign from malignant lesions will almost definitely require a biopsy. It can be sensible to point out these three diagnoses in cases involving multiple pleural lots or in depth pleural thickening. In this case, the extra presence of a big mediastinal mass suggests invasive thymoma with pleural involvement. Pleural metastatic disease is mostly secondary to lung or breast most cancers, indicators of which can be seen on the available chest imaging. Malignant mesothelioma is strongly associated with previous publicity to asbestos, however not all people uncovered to asbestos will develop mesothelioma (approximately 5%). The latent period between publicity and development of this situation is between 30 and forty five years. This is usually a large, easy, spherical mass, which can be pedunculated and cellular within the pleural area. Empyema is often unilateral, adjacent to an space of pneumonia/consolidation and may kind a convex border with the lung (lentiform shape). The "cut up pleura" sign of empyema refers to thickening and enhancement of the visceral and parietal pleura, separated by the purulent fluid. The adjacent gentle tissue of the chest wall may show indicators of irritation, such as thickening and stranding of the fat.
Inderal 40 mg cheap free shippingDespite rising interest arteria hypogastrica buy inderal 40 mg mastercard, adequate evidence of long-term efficacy of implanted peripheral nerve stimulation remains missing right now arterial blood pressure inderal 40 mg order free shipping. Botulinum toxin the use of botulinum toxin in neuropathic ache situations is growing in scientific practice. Its effectiveness in the therapy of situations corresponding to cervical dystonia, spastic circumstances, bladder overactivity, and hyperhidrosis are acquainted to most physicians [14]. Common purposes now embrace its use in continual migraine and occipital neuralgia. Direct analgesic results of botulinum toxin are postulated to involve impairment of sympathetic transmission and discount of neurogenic irritation [16]. Neurogenic irritation has been demonstrated after peripheral nerve damage and toxin may inhibit release of inflammatory mediators such as substance P, calcitonin gene associated peptide, and glutamate [17]. Interest in use of botulinum toxin has resulted in numerous human and animal mannequin studies. In their examine, both intrathecal and peripheral (intraplantar) administration of the neurotoxin resulted in decreased peripheral nerve injury, mechanical allodynia, and thermal hyperalgesia when saline-injected control mice had been in contrast with botulinum-injected mice. After a single injection, the treated group demonstrated fast (within 24 hours) improvement in mechanical allodynia and cold hyperalgesia. These neuromodulatory effects had been long lasting (81 days in mice) and will mirror enhancement of regenerative processes in the injured nerve models [18]. Placement of the electrodes can be carried out by open surgical procedure or percutaneous technique with ultrasound becoming increasingly widespread for placement of percutaneous leads. It has become an increasingly employed option in the treatment of neuropathic pain the place a stimulating lead is implanted alongside the pathway of the nerve to produce paresthesias similar to spinal twine stimulation. Established indications embrace neuralgias, post-traumatic and post-surgical neuropathies, and sophisticated regional pain syndromes. New indications continue to be explored together with potential makes use of in headache syndromes and fibromyalgia [13]. Peripheral nerve stimulation may be used in patients that may not be appropriate for spinal wire stimulation or other interventional procedures. Contraindications include unmanaged bleeding diathesis, ongoing anticoagulation, and 269 Section 6: the Management of Neuropathic Pain Wittekindt et al. It could additionally be a helpful tool in types of intractable neuropathic ache unresponsive to more conventional remedy [20]. Intrathecal drug delivery Intrathecal analgesia has a protracted historical past with many advances made in strategy of delivery and with discoveries of new indications. First studied had been the opioids [21], which turned an alternative therapy for persistent ache states in any other case refractory. Patients requiring intrathecal drug delivery are of two broad categories: (1) patients suffering from terminal sickness such as with malignancy, and (2) chronic non-malignant ache. Usually, a profitable intrathecal drug trial is accomplished before the drug supply system is internalized [22]. Intrathecal pumps ship very small medicine doses into the cerebrospinal fluid. The most typical medications delivered by implantable drug supply techniques include opioids, native anesthetics, adrenergic agonists, N-methylD-aspartate receptor agonists, and different agents [23]. Unfortunately, there are very limited scientific research available for evaluate of opioid efficacy, even though this is the most commonly delivered intrathecal medication. There has been a double-blind, randomized, crossover, multicenter study performed studying intrathecal bupivacaine supply along with intrathecal opioid supply. In another retrospective examine, patients failing intrathecal opioid delivery had bupivacaine added for intrathecal supply � here, considerably lower ache scores and a dosage discount in opioids ingested was famous [25]. Another randomized, double-blind, placebocontrolled examine evaluated intrathecal ziconotide in a big patient inhabitants [26]. This affected person population had important ache reduction with ziconotide compared with placebo with good tolerability using a slow titration. Systemic lidocaine Systemic lidocaine delivery has been used for many years for continual ache administration. Although once more affected by an absence of acceptable clinical trials, there are numerous clinicians utilizing lidocaine for patients with refractory or even for sufferers not essentially refractory to more conservative oral medications. First used for acute post-operative ache management [27], systemic lidocaine has not turn into widely accepted for acute ache management due to two reasons: (1) vital potential for cardiac and central nervous system opposed effects, and (2) other therapies similar to epidural anesthetic and/or a narcotic provide efficient acute pain management with more anticipated and manageable antagonistic effects. In a small study, intravenous lidocaine supplied larger, however transient, ache aid in comparison with placebo [28] for patients with peripheral neuropathic pain. Another similarly small research also demonstrated the power of intravenous lidocaine to provide greater ache relief than placebo for spinal cord damage pain [29]. Future research are required to better clarify safety, applicable dosing, and applicability to various neuropathic ache conditions in larger research populations. For most patient populations, refractoriness to different options should be clarified first, and willpower of potential safety in individual sufferers should always be thought-about. For offering very localized pain relief, interventional methods can be used to restrict adverse effects possible with oral medications, however the specialist should consider many components mentioned above earlier than continuing. Evidence-based guidelines for interventional pain medicine based on medical diagnoses. Pulsed radiofrequency therapy in interventional ache management: mechanisms and potential indications � a evaluate. Percutaneous radiofrequency lesion of the stellate ganglion in the therapy of ache in higher extremity reflex sympathetic dystrophy. Botulinum toxin sort A induces direct analgesic results in persistent neuropathic pain. Botulinum neurotoxin type A counteracts neuropathic ache and facilitates practical recovery after peripheral nerve damage in animal models. Botulinum toxin A for neuropathic ache after neck dissection: a dose-finding examine. Continuous low-dose intrathecal morphine administration in the remedy of continual ache of malignant origin. Intraspinal opioid remedy for persistent nonmalignant ache: current practice and medical guidelines. Polyanalgesic Consensus Conference 2003: an update on the administration of pain by intraspinal drug supply � report of an expert panel. Clinical experience with intrathecal bupivacaine in combination with opioid for the therapy of chronic pain related to failed back surgical procedure syndrome and metastatic most cancers pain of the backbone. A randomized, doubleblind, placebo-controlled research of intrathecal ziconotide in adults with extreme persistent ache. Inhibition of postoperative pain by continuous low-dose intravenous infusion of lidocaine. Neuromodulation controls pain, improves quality of life and practical standing, and reduces healthcare expenditures. In distinction to ablative procedures, neuromodulation is completely reversible and utilizes implantable devices that employ electrical energy or chemical agents that inhibit, excite, or modulate exercise of neuronal groups and networks in order to achieve therapeutic impact.
Inderal 40 mg discount without a prescriptionThis reflects both bone hypoplasia and the strain effects of intercostal neurofibromas blood pressure 300 inderal 40 mg order with visa. There can also be different related options of neurofibromatosis blood pressure medication for anxiety discount inderal 80 mg without prescription, as described earlier in this case. Superior rib notching is much less common and has a separate list of differential diagnoses. It is usually seen in conditions producing resorption of bone, corresponding to lateral clavicle resorption (see Case 23). Unilateral rib notching happens when there are differential pressures within the subclavian arteries. If the area of focal aortic stenosis lies proximal to the origin of the left subclavian artery, there will be unilateral right-sided rib notching. There are central endplate depressions in multiple thoracic vertebral bodies, which have a biconcave shape, consistent with H-shaped vertebrae. Other causes of diffuse osteosclerosis embrace sclerotic metastases, renal osteodystrophy, myelofibrosis and congenital conditions similar to osteopetrosis. If this can be a new analysis, I would inform the requesting clinician and counsel referral of the patient to the haematology staff for follow-up. Discussion Diffuse osteosclerosis is more than likely to be demonstrated in the examination on a chest, stomach or pelvic radiograph. The case shown is just one of several manifestations of sickle cell illness that may appear in an examination situation. Fluorosis is an extremely rare situation and has not made it into our mnemonic for that cause. Unless you see the obvious and attribute ligamentous calcification of fluorosis, this analysis must be mentioned with warning in the exam, after which only at the finish of your list of differential diagnoses. Examiners are more probably to appreciate a dialogue of the extra widespread conditions, such as renal osteodystrophy, metastatic disease, sickle cell disease and myelofibrosis. Pearls List the extra widespread differential diagnoses first: renal osteodystrophy, diffuse metastases, sickle cell illness and myelofibrosis. If current, think about sclerotic metastases and search for axillary clips, lung nodules and lymphangitis. Metastatic illness is commonly secondary to breast most cancers in females and prostate cancer in males. If the bones are strikingly and uniformly dense, contemplate congenital causes corresponding to osteopetrosis and pyknodysostosis. These have associated bone fragility, so look for deformities that indicate previous pathological fracture. The paediatric conditions on this listing may be differentiated utilizing a lateral movie of the cranium and mandible. A regular size sclerotic mandible with supernumerary teeth is present in osteopetrosis, whereas a hypoplastic sclerotic mandible related to a number of wormian bones is present in pyknodysostosis. There are multiple, well-circumscribed, lucent lesions inside each proximal femora and the pubic rami. There is a transcervical fracture of the left femoral neck, which is presumably pathological. In an grownup patient, the more than likely diagnoses are metastatic disease or a quantity of myeloma. Brown tumours is also thought of, particularly if there was any proof of hyperparathyroidism. To take this additional, I would review the earlier imaging and clinical history for evidence of recognized main malignancy. If available, hand radiographs might be assessed for proof of hyperparathyroidism. Serum and urine electrophoresis would determine paraproteins in preserving with myeloma. Raised calcium and parathyroid hormone ranges would suggest hyperparathyroidism and brown tumours. Discussion There is critical overlap in the appearances of the situations described right here. It is essential to point out these two possible causes in both a viva and long case examination setting. As well as presenting with diffuse skeletal involvement, as on this case, myeloma might current as a single lesion (plasmacytoma), diffuse skeletal osteopenia (especially seen within the spine, the place it usually presents with multiple wedge compression fractures) and, rarely, sclerotic bony lesions. It is difficult to distinguish between lytic metastases and myeloma on plain radiographs alone. A bone scan could additionally be abnormal in metastatic disease however shall be normal in cases of myeloma, which is assessed with a collection of plain radiographs often known as a "skeletal survey". Non-radiological checks can also be beneficial in your administration plan � for instance, urine and serum electrophoresis to look for the presence of monoclonal protein, as this is among the diagnostic criteria for myeloma. Fibrous tissue varieties within the medulla replacing the traditional trabeculae and creating a lucent lesion. The fibrous tissue progressively calcifies and develops a ground-glass look, progressing to a sclerotic rim ("rind" sign) with eventual sclerosis and resolution. Pearls Metastases and myeloma are at the prime of the list of differential diagnoses in an adult affected person and have a similar look on plain radiographs. Expansile lytic bone lesion "Politicians Always Make Grave Blunders" Condition P Plasmacytoma/large myeloma deposit Associated options Occurs in these aged >35 years old Well outlined Any location May be a number of lesions if a number of myeloma Occurs in these aged <30 years old Most widespread in lengthy bones across the knee, proximal femur and backbone Metaphyseal Well outlined Occurs in these aged >40 years old Well or ill-defined, however look for aggressive features May be a number of Any location Closed epiphysis Well-defined non-sclerotic margin Eccentric position Epiphyseal � the lesion must abut the articular floor Most commonly adjoining to the knee, the distal radius and sacrum Well outlined Any location Look for evidence of hyperparathyroidism. There is a solitary lucent and expansile lesion within the left ilium involving the left acetabulum. This has an ill-defined margin medially and a extra well-defined margin superiorly. There is destruction of the lateral cortex of the ilium and the superior margin of the acetabulum. Thyroid and renal carcinomas are frequent causes of expansile lytic metastases; nonetheless, breast and lung metastases are additionally attainable. In general, age is a helpful discriminator when forming a prognosis of a bone lesion. You can show your information by describing the age of the patient in your first sentence using a term corresponding to "adult", "youngster" or "toddler". Signs of degenerative joint illness are more doubtless to be current in older adults somewhat than in someone in their twenties or thirties. You also can describe the skeleton as "fused" or "unfused" to signify age, although that is much less particular. In this case, the margin of the lytic lesion has each nicely and ill-defined elements. The presence of an ill-defined margin (or, to put it another way, a wide zone of transition), whether or not full or not, suggests an aggressive process similar to metastatic illness. Pearls Always resolve whether a lesion is aggressive or non-aggressive � make this the primary assertion in your abstract. The primary feature determining whether a lucent lesion is aggressive is its margin or zone of transition � all the time comment on this.
Inderal 40 mg buy cheapPerhaps the single most necessary diagnosis to be created from an imaging examination carried out to consider cognitive deficits is the distinction of irregular and normal blood pressure 6020 buy inderal 40 mg low cost. This distinction may be challenging and the diploma of confidence will not be excessive heart attack ncla 80 mg inderal order visa, depending on the abnormality and the imaging modality. A regular examination has comparatively excessive negative predictive value and may be significantly reassuring. Many processes cause diffuse brain parenchymal volume loss, including continual systemic disease. In these circumstances, diffuse, symmetric brain atrophy involving the cerebrum, cerebellum, and brainstem normally is present. When atrophy is current, including each lateral asymmetry and uneven intrahemispheric lobar and sublobar abnormalities, suspicion of a neurodegenerative course of ought to enhance. Unfortunately, the superior levels of many cerebral cortical neurodegenerative processes are similar, with diffuse abnormality involving heteromodal association cortices within the frontal, parietal, and temporal lobes and relative, though not absolute, preservation of main somatic motor and sensory cortices. Consequently, the patient is evaluated for possible delirium, with neurodegenerative illness included among the diagnostic concerns. FrontotemporalDementia the principal molecular pathology of Lewy our bodies is -synuclein, which aggregates to kind abnormal intraneuronal inclusions known as Lewy bodies. The appearance of those circumstances is especially variable with respect to each the imaging findings and the medical presentation. Otherwise, this look is relatively nonspecific and could represent a late stage of Alzheimer disease, frontotemporal dementia, or Parkinson disease with dementia. Advanced dementia with Lewy our bodies may have this look, though less residual occipital lobe metabolic exercise may be present in that setting. Initial frontal lobe abnormality typically is principally medial or lateral and advances to turn out to be extra confluent. As the disease progresses, increasing involvement of other heteromodal affiliation cortices happens, including the parietal lobes, with relative sparing of the first somatic motor and sensory cortices. On imaging, Creutzfeldt-Jakob illness is distinguished by abnormality involving cortical and deep grey matter nuclei, sometimes in a patchy and uneven sample that might be unusual for other cerebral cortical neurodegenerative processes. The time course, earliest signs, amnestic versus nonamnestic quality, age, household history, motor deficits, and fee of development all play an necessary role in formulating a differential diagnosis that guides evaluation of imaging findings. A regular examination has good adverse predictive value relative to the development of dementia, whereas an abnormal examination, even if the sample is nonspecific, markedly increases the chance of an eventual analysis of a neurodegenerative disease. The rarity of this situation is expounded partly to the problem of sustaining a adequate number of small infarctions enough to substantially impair cognitive operate with out suffering a life-ending event. Consequently, its manifestations are regularly seen on examinations of aged sufferers which are carried out for indications aside from cognitive decline, similar to head trauma. In many circumstances, a dialogue between the radiologist and the referring physician could additionally be helpful in relaying findings which might be a trigger for concern and in discerning their relevance to the care of the affected person. Additionally, hypometabolism is present in the right thalamus and, to a lesser extent, in the right striatum. The relative hypometabolism within the left cerebellum represents crossed cerebellar diaschisis associated to the right frontal lobe abnormality. Note that the right and left thalami are roughly regular and symmetric in size and exercise. Common features of subcortical neurodegenerative problems include motion issues, dysautonomia, oculomotor nerve dysfunction, behavioral issues, and cognitive deficits. The mixture of these signs could recommend a selected prognosis, implicate considered one of a small number of disorders, or be totally nonspecific and defy simple classification. As with cortical neurodegenerative ailments, the history is an essential element within the interpretation of imaging examinations carried out for the evaluation of potential subcortical neurodegenerative illness, and it is necessary to derive a broad differential diagnosis from the clinical historical past to ensure that all related structures have been evaluated. In these circumstances, family historical past and bodily examination together could additionally be adequate for a confident analysis, and thus imaging regularly has little function within the diagnosis of these disorders. In other conditions, similar to when a patient presents with an atypical movement disorder with extrapyramidal features, no family historical past could also be pertinent and imaging may play a significant function in analysis. In many instances, motion disorders may be tough to characterize because the features could also be uncommon, troublesome to reproduce, and asymmetric with respect to laterality and upper and lower extremity involvement. Considerable overlap exists between subcortical and cortical neurodegenerative diseases, notably of their advanced stages, when symptoms of each varieties may be current. As with the cortical neurodegenerative ailments, historical past is an essential factor of analysis, and early symptoms and imaging findings could provide probably the most particular prognosis. However, confounding options might exist that forestall definitive prognosis on the basis of a clinical examination. Subcortical neurodegenerative diseases could have predominantly symmetric manifestations. Although asymmetric abnormalities could also be comparatively conspicuous, it could be difficult to discern a symmetric abnormality. As previously famous, the historical past is essential and should be used to formulate an inventory of constructions that require scrutiny, and this scrutiny should be applied whereas recognizing the big selection of regular appearance of subcortical buildings. Subcortical involvement is most evident within the thalamus and to a lesser extent in the striatum, and because the disease progresses, extra pronounced involvement of deep gray matter and brainstem buildings occurs. As the illness progresses, gaze palsies, cognitive deficits, speech disturbance, and swallowing issues turn out to be extra pronounced. The gaze palsy tends to be extra pronounced vertically, with downward palsy sometimes previous upward gaze palsy. Also observe the atrophy involving the middle cerebellar peduncles and cerebellum, with associated enlargement of the fourth ventricle. Depending on the genotype, degeneration might occur comparatively selectively throughout the cerebellum or spinal wire, and signs could include gait dysfunction, ataxia, dysarthria, and dysphagia. Although behavioral and cognitive deficits may be seen, many sufferers progress to endstage, terminal disease without marked cognitive deficits. Imaging findings sometimes replicate the region of involvement and may show abnormalities in the brainstem and cerebellum. Note that the pons is relatively preserved, forming the wings on the hummingbird and distinguishing this look from the extra diffuse brainstem atrophy which could be seen in other processes, similar to multiplesystem atrophy (see Case C, for example). Factors such because the time course, earliest symptoms, age, family historical past, and rate of development all play an necessary position in formulating a differential analysis that guides the analysis of imaging findings. Often the addition of medical historical past may focus the considerations, although in some instances a differential diagnosis could also be the finest possible interpretation. Magnetic resonance imaging can readily distinguish epidermoid cysts from arachnoid cysts. In addition, arachnoid cysts displace vessels and nerves, whereas these constructions can travel through epidermoid cysts. As their name implies, arachnoid cysts are space-occupying cystic lesions within the arachnoid area. They are slowly rising lesions that are inclined to insinuate themselves into the subarachnoid cisterns and sulci and therefore have lobulated, crenulated, and irregular margins. Epidermoid cysts may appear anywhere within the neural axis; nonetheless, the most common intracranial sites embody the cerebellopontine angle and the sellar region.
|