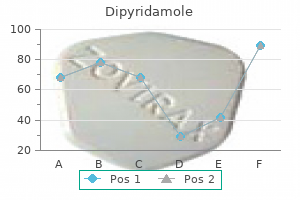
Generic dipyridamole 100 mg on lineBe nig n the rato ma (de rmo id cyst) Deriving from germ cells blood pressure when sick buy discount dipyridamole 25 mg line, benign teratom ata are relatively com m on blood pressure keeps rising dipyridamole 25 mg line. Thus the derm oid m ay contain hair, teeth and pultaceous m aterial from sebaceous glands. It m ay happen at any age, however m ostly is detected when the wom an is aged between 20 and 40. A painless cystic or stable m ass in the cul de sac, or within the position of an ovary, or Co nne ctive tissue ne o plasms Fibrom ata constitute 5% of benign ovarian neoplasm s. Small (16 mm), wellcircumscribed echogenic (bright) lesion surrounded by normal (darker) ovarian tissue. In youthful wom en ovarian cystectomy is possible, 303 Fundam entals of Obstetrics and Gynaecology the ovary being reconstructed after the tum our has been shelled out. A sim ilar method can be utilized in instances of serous cystadenom a, but in wom en over the age of forty bilateral salpingo oophorectomy and whole hysterectomy is preferred, due to the potential of m alignant change. Endom etriom ata, benign teratom ata and brom ata can often be shelled out of the norm al ovarian tissue and the ovary reconstructed. If an ultrasound examination ination of the pelvis is m ade routinely, ovarian tum ours are detected in 1 in 200 preg nancies. Most of them are cysts, normally an enlarged corpus luteum which resolves spontaneously. Most are serous cystadeno m as, a number of are m ucinous cystadenom as, and these two account for 65% of all neoplasias com plicating pregnancy. Teratom ata account for 25% and the rem aining 10% is m ade up of a broad variety of ovarian tum ours. Rarely, torsion of the ovary con taining the tum our m ay occur and, even m ore not often, the tum our m ay rupture. T atme nt re Treatm ent is determined by the size and consistency of the tum our and its ultrasound look. Ovarian tum ours <80 m m in diam eter and echo free can be observed, repeat scans being m ade to see if the tum our increases in dimension. If treatm ent is decided upon, the cyst m ay be aspi rated or a cystectomy carry out ed. A m ultilocular cyst or a tum our >80 m m in size which is thick walled or sem isolid requires surgical rem oval after the 12th gestational week. A tum our detected after the 30th gestational week m ay be dif cult to rem ove surgically and prem ature labour m ay follow. The determination to operate can solely be m ade after careful consideration and involvem ent of the patient and her partner. Diag no sis In early pregnancy a vaginal examination ination m ay reveal two m asses, the pregnant uterus and the ovarian tum our. Superior to it is a layer of basal cells from which the other cell layers differentiate. The interm ediate cell layer consists of large cells, each with reticulated nuclei and vacuoles of glycogen within the cytoplasm. This proportion is larger if the wom an or her companion has had several sexual companions. In m ost cases the infection is sym ptom much less and disappears inside a couple of m onths (see p. Possible cofactors in cervical carcinogenesis embrace cigarette sm oking, im m unosuppression, horm onal elements and vitam in de ciencies. A num ber of countries provide the vaccination from age 12�13 as a lot as 27 years, and likewise to younger m en earlier than they becom e sexually lively. These can be detected by m icroscopically exam ining an exfoliative cervical sm ear, stained using the Papanicolaou stain (the Pap test). The proportion of falsenegative sm ears will be lowered if strict standards are adopted for taking and for exam ining the sm ear. A further re nem ent is liquid-based cytology that includes taking cervical cells with a Cervex sam pler brush and rinsing the comb into a vial of xative. This m ethodology reduces the unsatisfactory/inconclusive sm ear fee by 80% and has been shown to be cost-effective. The approach has the potential to be used for the detection of other sexually transm itted ailments, such as chlamydia and gonorrhoea. During the reproductive years the tremendous cial cells are continually shed or exfoliated into the vagina, and differentiation of cells from the basal layer also proceeds continuously. In som e wom en the nuclei becom e abnorm ally formed or dyskaryotic, which m ay indicate a precancerous change; this can be detected by cervical sm ears. There is powerful m olecular 306 Chapter 3 7 Prem alignant and m alignant situations of the fem ale genital tract for abnorm al cells. The advantage of this strategy is that rescreening only has to be undertaken each 5 years as it has been proven to be as protected as screening each 2�3 years with the Pap check. The nuclei are distorted by the effects of vaginal infections, such as trichom oniasis and Gardnerella. The referring physician is requested to deal with the infection appropriately and then to repeat the sm ear. A Cervex-Brush is shaped to take sam ples of cells from the endocervix and ectocervix. Before perform ing a vaginal examination ination, both the good and cozy ed m etal speculum or a plastic speculum is inserted to expose the cervix. The Cervex-Brush is inserted into the cervical canal and rotated one to one and a half tim es. Glandular cell � Endom etrial cells cytologically benign in a � � postm enopausal wom an Atypical glandular cells of undeterm ined signi cance Adenocarcinom a � Endocervical � Endom etrial � Extra-uterine � Not in any other case speci ed. If an abnorm al sm ear is reported, the necessity to counsel and clarify is im perative. To m any wom en, the nding of a dyskaryotic sm ear suggests the presence of cancer. Repeat the cervical sm ear in 12 m onths: if the abnorm ality persists refer for colposcopy; if this sm ear is reported as norm al repeat in 12 m onths. There is, nevertheless, no proof from random ized managed trials that this early intervention conveys any bene t over option 1. A educated observer can differentiate between the m inor and m ajor cervical precancer lesions and carcinom a with an inexpensive degree of accuracy. The predicted diagnosis is con rm ed by punch biopsies, that are examination ined histologically. Local destructive treatm ent contains laser, cryosurgery and electrocoagulation diathermy.
Syndromes - Being around certain chemicals
- Anticholinergics
- Developmental and genetic conditions that were present at birth
- Malnutrition
- Vomiting
- What other symptoms are present?
- Common peroneal nerve dysfunction
- Drug abuse
Cheap 100 mg dipyridamole overnight deliveryReasons of air flow embody hemodynamic instability heart attack youtube cheap dipyridamole 100 mg on line, insufficient restoration arteria umbilical dipyridamole 25 mg cheap fast delivery, hypothermia, or other intraoperative problems. Hypertension could make surgical procedure more difficult and will increase the chance of submit operative hemorrhage. A throat pack is recommended and ought to be included within the swab depend to guarantee removal prior to extubation. Extubation or elective mechanical ventilation Patients ought to be extubated in lateral position to forestall airway soiling or awake within the sitting position to minimise additional bleeding and maximize post operative oxygen trade. A mixture of infusions of propofol (75�150 g/kg) with isoflurane/ sevoflurane/desflurane (0. Extubation: in patients with stable hemodynamics and preserved cranial nerve functions. Elective ventilation: in patients with decrease cranial nerve palsy, prolonged surgery, huge blood loss, and hypothermia. Postoperative considerations Mechanical ventilation, decrease cranial nerve dysfunction leading to aspiration, publicity keratitis (if facial nerve injury). Toxicology panel (ethanol, tricyclic antidepressants, urine, and blood toxicology screen). Peripheral arterial entry for invasive blood stress monitoring during highdose midazolam infusion or pentobarbital coma. Arterial blood stress monitoring for high-dose midazolam infusion or pentobarbital coma. Alternate/subsequent second line: phenytoin (if fosphenytoin not available), levetiracetam, phenobarbital, valproate, lacosamide. Third line (anesthetics delivered by steady infusion): high-dose midazolam, pentobarbital. For these with no history of seizure however likelihood of future seizures, consider upkeep levetiracetam or fosphenytoin for seizure prophylaxis. Protect the affected person from injuring the top or extremities by falling or hitting in opposition to the bedrails. Recovery position will assist keep airway however transition to positioning for efficient bag-mask air flow could additionally be required. Thiamine concurrently for hypoglycemia in adults to stop Wernicke�Korsakoff syndrome in the scenario of persistent alcohol intoxication. Consider a short-acting muscle relaxant for intubation as clinical seizures might be masked throughout chemical paralysis. Once seizures and their underlying causes have been controlled the patient could additionally be allowed to wake up and extubate. Induce fentanyl/propofol/rocuronium or atracurium or speedy sequence induction with succinyl choline (full stomach). To facilitate easy and fast emergence from anesthesia to allow early neurological assessment. Others (optional): neurophysiological monitoring, jugular venous bulb oxygen saturation. To avoid fluctuations in cerebral perfusion pressure that may lead to everlasting brain damage. Preoperative medications prescribed prior to surgery, corresponding to carbonic acid anhydrase or other medications that are usually used to deal with intracranial hypertension, could additionally be continued on the discretion of the treating doctor. Anticonvulsant (antiepileptic) medications prescribed to treat underlying epilepsy dysfunction have to be continued. Anticonvulsants can also be prescribed prophylactically, on the discretion of the treating physician. Once intubated, the endotracheal tube is mounted and eyes should be taped to avoid inadvertent corneal abrasions intraprocedurally. Oxygenation: the affected person is ventilated with oxygen at different fraction of inspired oxygen (FiO2) (at the discretion of the anesthetist) to present normoventilation or mild hyperventilation and normal oxygenation. Different anticonvulsants corresponding to valproate, levetiracetam, phenytoin, or lacosamide may be used. For mild-to-moderate analgesia, one can administer acetaminophen 650 mg every 6 h, however not to exceed 4000 mg each 24 h. For moderate-to-severe analgesia, one can use fentanyl 25�100 g depending on the ache severity. If repeated doses of fentanyl are used, one will want to monitor psychological status and airway. Postoperative considerations Hemorrhage, postoperative wound dehiscence, electrolytes disturbance, seizure, shunt infection, shunt malfunction, and shunt failure/migration. Although it was reported to happen extra commonly in sitting positions, air embolism could happen in any surgical position, including susceptible, as lengthy as a gradient develops between the operation web site and the heart. The main air emboli usually originates from noncollapsible cerebral venous sinuses, principally the transverse, sigmoid, and the posterior half of sagittal sinus, through venous channels in the diploic space throughout the cancellous bone of cranium (which may happen throughout craniotomy and also pin fixation). Air might enter by way of emissary veins, which may be opened to atmosphere at their level of entry to the occipital bone, during procedures requiring dissection of suboccipital muscle. The intradural venous channels are regularly opened, but is probably not coagulated effectively as a end result of the confined area of burr holes. The pathophysiologic consequence of gradual air infusion is totally different from that of large air emboli, as a end result of small air bubbles cross via the right coronary heart to lodge within the pulmonary vasculature, resulting in mechanical obstruction to pulmonary blood flow. The consequences of the effects of air emboli most commonly depend upon quantity and rate of accumulation. This passage is more prone to occur in the presence of enormous volumes of air in the pulmonary vascular filter. Pulmonary vasodilators and inhalational anesthetic brokers may decrease the brink for the air passage. Hyperbaric O2 remedy could additionally be of benefit on this state of affairs by reducing the bubble dimension. Despite this modified semi-sitting position, these patients require particular monitoring to provide a safer surgical procedure. The diploma of the head-up position in accordance with the surgical process should be an important issue for the choice to omit or go for a proper coronary heart catheter. These locations might nicely serve for optimum recovery from small volumes of air emboli when cardiac output is properly maintained. The proper heart placement could be verified by either radiography or intravascular electrocardiography. Hence, minor events revealing no scientific indicators or signs may not be detected by utilizing routine monitoring strategies and may remain unnoticed in routine follow. In addition, the amount of air must also be detected to anticipate the prognosis. A "washing machine" or "drum-like" sound can be utilized as an early signal to detect air embolus; nonetheless, it requires an experienced, dedicated technician and may show false-positive results during electrocautery. The mechanism of cough has not been clearly established but; nonetheless, it may be because of bronchial irritation caused by pulmonary venous congestion. In both conditions, all measures have been recommended to be taken to prevent worsening of the occasion.
25 mg dipyridamole saleThese embrace rupture of a deep cerebral finish artery hypertension signs and symptoms treatment dipyridamole 100 mg buy cheap, amyloid angiopathy blood pressure medication edema cheap 100 mg dipyridamole with amex, mycotic aneurysm, arteriovenous malformation, or hemorrhage right into a tumor, and every requires a unique clinical approach. Rupture of deep cerebral finish arteries normally occurs in sufferers with long-term, poorly handled hypertension; it may possibly additionally complicate diabetes or different types of atherosclerotic arteriopathy. The blood vessels which are most probably to hemorrhage are the same ones that cause lacunar strokes. We will deal with the primary two, which trigger supratentorial masses, on this section, and the latter two within the section on infratentorial lots. Capsular or basal ganglionic hemorrhages sometimes current with the acute onset of hemiplegia. Thalamic hemorrhage may current with sensory phenomena, but often the hemorrhage compresses ascending arousal methods early in order that lack of consciousness is the first presentation. Obtundation is from swelling of the infarcted tissue, progressing to stupor in 12�24 hours, coma often in 36�96 hours. Conjugate gaze paresis to facet of motor weakness; contralateral oculovestibular responses could be suppressed for 12 hours or so. Contralateral hemiplegia, usually with extensor plantar response and paratonia ipsilateral to lesion. Sudden-onset headache, adopted by roughly quickly evolving aphasia, hemiparesis to hemiplegia, conjugate ocular deviation away from hemiparesis. Clinical image just like frontoparietal hemorrhage but seizures uncommon, vomiting frequent, eyes characteristically deviated down and laterally to either side. Sudden onset of coma or speechlessness, pinpoint pupils, ophthalmoplegia with absent or impaired oculovestibular responses, quadriplegia, irregular respiration, hyperthermia. Acute and rapid onset and worsening inside hours of occipital headache, nausea and vomiting, dizziness or vertigo, unsteadiness, dysarthria, and drowsiness. Small and reactive pupils, nystagmus, or horizontal gaze paralysis towards the aspect of the lesion. Midline and ipsilateral ataxia, ipsilateral peripheral facial palsy, and contralateral extensor plantar response. Vertigo, ataxia, nausea, uninteresting headache, nystagmus, dysarthria, ipsilateral dysmetria; 24�96 hours later: drowsiness, miosis, ipsilateral gaze paresis and facial paresis, worsening ataxia, extensor plantar responses. Acute Subarachnoid Hemorrhage Awake at onset, sometimes hypertensive, sudden headache, usually adopted within minutes by unconsciousness. Subhyaloid hemorrhages, hemiparesis or aphasia could or will not be present, hemisensory modifications rare. Miller Fisher tried to identify the arteries that had brought on lacunar infarctions in postmortem examination of the mind. Given the fact that such vessels sometimes take off at a right angle from large cerebral arteries, one may anticipate excessive shearing forces at the vessel origin, so that hypertension or other atherosclerotic risk components would possibly cause earlier or more severe injury. End artery hemorrhages sometimes produce a big hematoma with appreciable local tissue destruction and edema. Because a lot of the scientific appearance is as a result of of the mass impact of the blood, which eventually is resorbed, the affected person may initially be rather more neurologically impaired than can be attributable to a comparably sized infarct. However, if the patient can be supported by way of the initial event, restoration is usually a lot greater than might be initially anticipated, and the hematoma is resorbed, leaving a slit-like defect within the mind. Amyloid angiopathy results from deposition of beta-amyloid peptide in the walls of cerebral blood vessels. Because amyloid deposits occur alongside blood vessels as they penetrate the cerebral cortex, the hemorrhages are usually lobar. As with end artery hemorrhages, the severity of the initial presentation typically is deceptive, and, as the hemorrhage is resorbed, there could also be much larger return of function than in a affected person with a equally positioned infarction. The wall of the blood vessel is colonized by micro organism, leading to aneurysmal dilation a quantity of millimeters in diameter. These aneurysms, which can be visualized on cerebral angiography, may be multiple. Because there may be a number of mycotic aneurysms, and to eliminate an arteriovenous malformation or saccular aneurysm because the supply, an angiogram is generally necessary. Unruptured mycotic aneurysms are treated by antibiotics, however ruptured aneurysms may require endovascular or open surgical intervention. They range from small cavernous angiomas to large arteriovenous malformations which are life-threatening. The irregular vessels in these malformations are thin-walled, low-pressure, and low-flow venous channels. Cavernous angiomas of the brainstem may cause coma in the event that they hemorrhage; the affected person often recovers, but these angiomas have a tendency to rebleed. Hemorrhage into a tumor sometimes occurs within the setting of a affected person with identified metastatic most cancers. Intracerebral Tumors Both major and metastatic tumors may invade the brain, leading to impairment of consciousness. In different circumstances, the patients could present with focal or multifocal indicators of cerebral dysfunction. As they enlarge, astrocytomas may outgrow their blood supply, resulting in inner areas of necrosis or hemorrhage and formation of cystic components. Impairment of consciousness is usually because of compression or infiltration of the diencephalon or herniation. Surprisingly, major brainstem astrocytomas, 4 Specific Causes of Structural Coma 147 which are usually seen in adolescents and younger adults, cause mainly impairment of cranial motor nerves whereas leaving sensory operate and consciousness intact till very late in the course. They typically occur alongside the ventricular surfaces and will infiltrate alongside white matter tracts. Metastatic tumors are most often from lung, breast, or renal cell cancers or melanoma. Unlike primary brain tumors, metastases rarely infiltrate the mind and can typically be shelled out at surgical procedure. This tendency also leads to tumors outgrowing their blood supply, leading to infarction and hemorrhage (see previous section). However, some antiepileptic medicine, similar to phenytoin or phenobarbital, could cause erythema multiforme in patients receiving cranial radiation, so are best avoided. Brain Abscess and Granuloma A wide selection of microorganisms, together with viruses, micro organism, fungi, and parasites, can invade the brain parenchyma, producing an acute damaging encephalitis (see page 156). However, if the immune response is profitable in containing the invader, a more continual abscess or granuloma could result, which may act more as a compressive mass. The infective agents reach the mind hematogenously or by direct extension from an infected contiguous organ (paranasal sinus, center ear). In many countries in Central and South America, cysticercosis is the most common reason for infectious mass lesions within the cerebral hemispheres. However, cysticercosis sometimes presents as seizures and only sometimes as a mass lesion.
Purchase 100 mg dipyridamole free shippingSerologic profile of myasthenia gravis and distinction from the Lambert� Eaton myasthenic syndrome blood pressure infant normal value dipyridamole 100 mg line. Clinical trial of plasma change and high-dose intravenous immunoglobulin in myasthenia gravis blood pressure monitor costco buy discount dipyridamole 25 mg online. Vecuronium dose-response and upkeep necessities in sufferers with myasthenia gravis. Etiology, mechanisms, and anesthesia implications of autoimmune myasthenia gravis. Mechanical ventilation for respiratory failure in myasthenia gravis: Two 12 months experience with 22 patients. Anaesthetic management of a patient with myasthenia gravis for abdominal surgery utilizing sugammadex. These include Campylobacter jejuni, cytomegalovirus, influenza virus, Epstein�Barr virus, and Mycoplasma pneumoniae. The scientific presentation usually begins with onset of sensory signs in the decrease limbs adopted by a fast onset flaccid paralysis. Progression is usually rapid with almost half of sufferers reaching peak weak point by 2 weeks and more than 90% of patients by the end of 4 weeks. The weak point is extra 449 450 Guillain�Barr� syndrome in distal muscular tissues compared to proximal muscles. More than two-thirds of patients are nonambulatory during weakness10; patients also complain of moderate-to-severe muscular pain. Neurological examination reveals widespread hyporeflexia or areflexia with distinguished distal weak point in comparison with proximal muscle tissue. Sensory examination might usually be regular with only lack of vibration and proprioception senses. Respiratory involvement Facial and laryngeal muscular tissues reflect the involvement of cranial nerves. In roughly 50% of patients, autonomic disturbance is noticed and is a big cause of death. These embody acute onset of tachycardia and hypertension, but critical life-threatening arrhythmia also can happen through the course of sickness. Electrodiagnostic testing: Electrodiagnostic testing is performed to support the prognosis of flaccid paralysis due to peripheral neuropathy. The features of demyelination embody slow conduction velocities, temporal dispersion, and increased latencies. The injury may be demyelinating, axonar degeneration with or without sensory involvement. Pathophysiology Destruction of myelin sheath by leukocyte infiltration Demyelination of motor neurons. Poor consequence Characterized by a triad of sensory ataxia, areflexia, and ophthalmoplegia. Approximately 30% of patients develop respiratory failure and require mechanical ventilation. Routine monitoring should embody heart rate, respiratory rate, effort of breathing, use of accent muscles of respiration, and signs and signs of autonomic dysfunction. A important capability of <20 mL/kg or a adverse inspiratory pressure of <30 cmH2O or a maximal expiratory strain <40 cmH2O signifies an imminent respiratory failure and is an indication for endotracheal intubation and mechanical ventilation. If the patient fails to show vital improvement in 2 weeks, then tracheostomy can be carried out. Side effects are often gentle and could be restricted to headache, nausea, and again ache. This course of removes humoral antibodies, immune complexes, cytokines, complement, and other inflammatory mediators. The earlier two studies from American and French groups, which included patients with plasmapheresis inside 2 weeks of onset of signs, confirmed a sooner motor recovery, time to walk, and speedy weaning from mechanical ventilation. One hundred percent oxygen earlier than suctioning reduces the incidence of bradyarrhythmias. The infusion should be began slowly at Deep vein thrombosis and ache administration A nonambulatory patient is at risk for developing deep vein thrombosis and subsequent References 453 pulmonary embolism. Low molecular weight heparins are the preferred medicine for the prevention of deep vein thrombosis in these patients. A majority of sufferers complain of back and lower extremity ache and must be handled aggressively. Guillain� Barr� syndrome: A prospective, populationbased incidence and consequence survey. Sur un syndrome de radiculo-nevrite avec hyperalbuminose du liquidecephalorachidien sans response cellulaire. The spectrum of antecedent infections in Guillain�Barr� syndrome: A case� control examine. Cytomegalovirus an infection and Guillain�Barr� syndrome: the medical, electrophysiologic, and prognostic features. Efficiency of plasma change in Guillain� Barr� syndrome: Role of alternative fluids. Repeated vital capability measurements as predictive parameters for mechanical ventilation want and weaning success within the Guillain�Barr� syndrome. Quantitative assessment of cardiovascular autonomic operate in Guillain�Barr� syndrome. Acquired inflammatory demyelinating polyneuropathies: Clinical and electrodiagnostic options. Clinical and electrophysiological predictors of respiratory failure in Guillain�Barr� syndrome: A prospective examine. Practice parameter: Immunotherapy for Guillain�Barr� syndrome: Report of the Quality Standards Subcommittee of the American Academy of Neurology. Guillain� Barr� syndrome in childhood: Natural course and efficacy of plasmapheresis. Cost evaluation of plasma-exchange remedy for the remedy of Guillain�Barr� syndrome. Beneficial results of plasma trade in acute inflammatory polyradiculoneuropathy. A randomized trial evaluating intravenous immune globulin and plasma change in Guillain�Barr� syndrome. Randomized trial of plasma trade, intravenous immunoglobulin and mixed treatments in Guillain�Barr� syndrome. Treatment of Guillain�Barr� syndrome with high-dose immune globulins combined with methylprednisolone: A pilot research. Seizures occur because of an imbalance between excitatory and inhibitory neurotransmission that favors excitation. A seizure that has continued for 2�3 min is rare, turns into more and more less prone to cease spontaneously, and ought to be treated.
25 mg dipyridamole generic overnight deliveryUse of nocturnal penile tumescence and rigidity in the evaluation of male erectile dysfunction blood pressure medication yellow teeth purchase dipyridamole 25 mg with mastercard. Erectile dysfunction is a strong predictor of poor high quality of life in males with Type 2 diabetes mellitus blood pressure medication starting with a buy generic dipyridamole 100 mg line. Efficacy and security of oncedaily tadalafil in males with erectile dysfunction who reported no successful intercourse makes an attempt at baseline. Rationale for mixture therapy of intraurethral prostaglandin E(1) and sildenafil in the salvage of erectile dysfunction patients desiring noninvasive therapy. Systemic pharmacokinetics of papaverine and phentolamine: Comparison of intravenous and intracorporal application. Intracavernosal injection remedy and surgical therapy in diabetic sufferers with erectile dysfunction. Intracavernosal alprostadil is efficient for the treatment of erectile dysfunction in diabetic males. High attrition rate with intracavernous injection of prostaglandin E1 for impotency. Patient acceptance of and satisfaction with an exterior adverse stress gadget for impotence. Outcome of penile prosthesis implantation for treating erectile dysfunction: expertise with 504 procedures. Beneficial impact of train and weight problems interventions on erectile perform and its threat factors. Sildenafil citrate, a selective phosphodiesterase kind 5 inhibitor: analysis and clinical implications in erectile dysfunction. Vardenafil, a new phosphodiesterase kind 5 inhibitor, in the therapy of erectile dysfunction in men with diabetes: a multicenter double blind placebocontrolled fixeddose research. Erectile dysfunction and diabetes: a evaluate of the present evidencebased drugs and a synthesis of the primary available therapies. New therapy choices for erectile dysfunction in patients with diabetes mellitus. Sildenafil for therapy of erectile dysfunction in men with diabetes: a randomized managed trial. The efficacy and tolerability of vardenafil, a new, oral, selective phosphodiesterase kind 5 inhibitor, in patients with erectile dysfunction: the first athome scientific trial. Impact of diabetes mellitus on the severity of erectile dysfunction and response to remedy: analysis of data from tadalafil clinical trials. Evaluation of the efficacy and security of onceaday dosing of tadalafil 5 mg and 10 mg in the remedy of erectile dysfunction: results of a multicenter, randomized, doubleblind, placebocontrolled trial. Efficacy of tadalafil once daily in men with diabetes mellitus and erectile dysfunction. Quantifying danger of penile prosthesis an infection with elevated glycosylated hemoglobin. Coated implants and "no touch" surgical technique decreases danger of infection in inflatable penile prosthesis implantation to zero. ChaPter 23 Management of erectile dysfunction in neurological patients Katarina Ivana Tudor1 and Jalesh N. Intact peripheral innervation by way of sympathetic and parasympathetic fibers derived from the hypogastric and pelvic plexuses conveys alerts liable for the neurological control of the erectile response. Reflex erections are mediated by sacral segmental pathways and end result from genital stimulation. The reflex erection is brief lived and usually insufficient for penetrative intercourse. Psychogenic erections originate from cortical and subcortical centers and are mediated through the thoracolumbar sympathetic outflow. In well being, these two merge together resulting in an erectile response enough for penetration. Neurological deficits ensuing from the disease can contribute to sexual dysfunction (secondary factors). Spasticity may find yourself in problem in assuming positions conducive to intimacy and sexual intercourse. Finally, factors corresponding to nervousness, despair, and guilt ensuing from having a neurological dysfunction can affect the connection and have an impact on sexual activity (tertiary factors)6,13�19 (Table 23. Additionally, medicines used in the administration of signs ensuing from neurological illness can affect sexual features; examples are antidepressants, baclofen, and gabapentin17 (Table 23. However, a crosssectional study in 1997 found that 47% of grownup longterm survivors of primary mind tumors exterior the hypothalamicpituitary area additionally Male Sexual Dysfunction: A Clinical Guide, First Edition. Fortytwo percent of the sufferers confirmed both evidence for hypothalamic hypogonadism (32%) or main gonadal damage (10%). Moreover, antihypertensive brokers generally utilized by stroke patients, corresponding to beta blockers, could lead to diminished cavernosal artery pressures and erectile dysfunction. This was significantly more frequent following rightsided temporal lobe resections, and more incessantly reported in females than males. In a bunch of men underneath sixty five years, 82% spontaneously regained erectile operate inside approximately 7 weeks following the stroke. Social life is affected in both headache types, as a end result of sensitivity to stress elements, degradation in quality of life, and workforce loss in communities. Though the most common manifestations are motor disabilities resulting in slowness and falls, nonmotor signs such as neuropsychiatric, sleep, sensory, and autonomic signs are recognized as being outstanding complaints impacting quality of life. Men with an entire lesion beneath S2 may have psychogenic erections however no reflex erections, but damage to the cauda equina results in almost full lack of erectile responses. Despite trendy treatment and improvement in intensive care amenities, the mortality stays static at 5%, with practically 20% of sufferers having persistent incapacity. Atherosclerosis is significantly accelerated because of hypertension, diabetes, inflammation, secondary hyperparathyroidism, and the impression of uremic toxins on the vascular endothelium. Twothirds of cases are related to antecedent an infection, which varies by geographical location. The infective agents implicated embrace Campylobacter jejuni, cytomegalovirus, Epstein�Barr virus, and Mycoplasma pneumoniae. Nurses had been considered as probably the most acceptable member of the healthcare staff to initiate a dialogue on sexuality and sexual problems. The purpose for such divergent findings is unclear; nonetheless, variations in affected person selection may have contributed. Patients utilizing sildenafil citrate have been more likely to improve their capability to achieve and preserve an erection and complete intercourse. Adverse events were additionally reported; the most typical were: headache, flushing, rhinitis, visible disturbances, and dyspepsia, however two patients suffered severe antagonistic events together with one with coronary artery illness requiring triple bypass surgery and one with a cerebrovascular accident. Neurological functions, such as handbook dexterity, have to be thought-about when discussing this option with the neurological affected person. Surgical implantation of a penile prosthesis should be thought-about with warning and a proper neurological examination is paramount as patients with perineal sensory loss are at a greater threat for issues similar to pores and skin erosion. Sexual difficulties for persons with a quantity of sclerosis in New South Wales, Australia.
Aetheroleum Pelargonii (Rose Geranium Oil). Dipyridamole. - Diarrhea, nerve pain, and use as an astringent.
- Dosing considerations for Rose Geranium Oil.
- How does Rose Geranium Oil work?
- Are there safety concerns?
- What is Rose Geranium Oil?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96190
Buy dipyridamole 100 mg onlineOther surgeons pre serve a half of the prepuce attached to the glans penis utilized in clitoroplasty to obtain an analogous impact heart attack jaw pain right side dipyridamole 100 mg order mastercard. Even when the complete penile skin tube is used for the vagina heart attack from weed dipyridamole 25 mg without a prescription, small labia minora could also be produced, with or without a second stage. Bleeding and labial hematoma Bleeding occurs in 10% of cases,29 regardless of meticulous method, and usually arises from the corpus spongio sum surrounding the urethra. Bleeding may be arrested by manual pressure and solely rarely requires return to theater but might necessitate administration of blood merchandise. It can also manifest as a labial hematoma, which could be managed conservatively but might improve the risk of wound dehiscence. Urethrostomy the only method of forming the urethrostomy is to divide the urethra within the bulb, and anastomose the skin to the urothelium. This, nevertheless, has a excessive incidence of subsequent urethral meatal stenosis, and in addition tends to lead to antegrade micturition. The different drawback is that the corpus spongiosum is essentially untouched, which leads to a bulge behind the urethra, which grows on arousal. In addition to trying unsightly, this can hinder the vaginal introitus throughout intercourse. For this cause, most surgeons will spatulate the urethra, and resect a number of the erectile tissue that surrounds it. The result ing wide anastomosis to the perineal skin has a a lot lower fee of stenosis, and the moist urethral epithelium provides a really passable beauty outcome. This comes with an elevated risk of bleeding within the forty eight hours after surgical procedure, however this can almost all the time be managed conservatively. During creation of the neovagina cavity, connective tissue is stripped from the entrance wall of the rectum at the junction between two arterial provides: the inferior mesenteric artery above and the hemorrhoidal vessels under. Damage to this "watershed" area may trigger breakdown or thinning of rectal mucosa on this area. This would explain why a misdirected dilator pushed by a patient into an 320 Chapter 33 proper dilation regime may also lead to lack of each vaginal width and depth. Hair progress will happen if scrotal pores and skin is used and the pores and skin has not been subjected to depilation, either pre or perioperatively. Once hair development is seen within the vault of the neovagina, little can be done to forestall its continued growth, and a variety of sufferers must return at intervals for elimination of hairballs. Neovaginal stenosis is reported in 4�10% of sufferers after a mixed penilescrotalskininversion technique. Sacrospinous ligament fixation has been reported to prevent this at 5year followup,41 however this does require careful preparation and placement of the anchoring sutures to stop rectal and vascular harm. Hyposensation of the neoclitoris34 and neoclitoral necrosis42 have been reported in the literature. As a result, a dilator with a ventrally pointing tip has been beneficial to keep away from this problem. If a fistula does develop, a defunctioning colostomy will enable 50% of fistulae to heal, the remainder requiring additional surgical procedure, with a few tough circumstances requiring elimination of the neovagina. Lower urinary tract issues Commonly reported functional urinary issues after vaginoplasty embody stress urinary incontinence or urgency signs (66%), obstruction (33%), and urinary tract infections (2%);24,34,36�39 these could additionally be handled as in natal females. Bellringer, unpublished work), with patients usually presenting 2 months after primary surgery, initially with discount in urine circulate, and then dribbling incontinence from persistent retention of urine. These patients require revision of the meatus, which is normally efficient, although a couple of do go on to longterm intermittent catheterization. Progressive obstructive voiding dysfunction due to meatal stenosis was reported as a major complication of penile inversion vaginoplasty. Followup and affected person satisfaction Satisfaction in a sometimes demanding patient population must fulfill each cosmetic and practical standards: esthetic appearances similar to the natal female genitalia; enough neovaginal depth and neoclitoral sensation to obtain orgasm; lubrication and lack of neovaginal pain43 � these are all factors that must be thought-about. Loss of depth could result from pores and skin loss, and correction of this often necessitates enterovaginoplasty. Some centers use belly pores and skin grafts on this circumstance, and a modification of the Davidov technique (originally described for the therapy of vaginal agenesis in natal women) has additionally been described. Failure to observe a Assessment and management of the male to feminine transgender patient with the functioning and beauty appearance of their genitalia. Eight sufferers (33%) reported regular sexual intercourse, and one hundred pc of their sufferers have been happy with neovaginal functionality, consequence, and beauty results. Neoclitoral sensation was glorious in 18 patients (78%), good in 5 (19%), and unsatisfactory in one patient. A sex distinction within the hypo thalamic uncinate nucleus: relationship to gender id. Prolactin ranges and pituitary enlargement in hormone treated maletofemale transsexuals. A methodology of preserving the glans penis as a clitoris in sex conversion operations in male transsexuals. Gender iden tity disorder: general overview and surgical remedy for vaginoplasty in maletofemale transsexuals. Aetiology and administration of rectovaginal fistulas following male to feminine gender reassignment. A case of profitable administration of recurrent bacterial vaginosis of neovagina after male to female gender reassignment surgery. Sacrospinous ligament fixation for neovaginal prolapse prevention in maletofemale surgical procedure. Corona glans clitoro plasty and urethropreputial vestibuloplasty in maleto feminine transsexuals: the vulval aesthetic refinement by the Andalusia Gender Team. Longterm assessment of the physical, psychological, and sexual well being amongst trans sexual ladies. Thirty years of International Followup Studies after Sex Reassignment Surgery: A Comprehensive Review, 1961�1991. Refinements of pre, intra, and postoperative care to stop issues of vaginoplasty in male transsexuals. Feminizing genitoplasty in grownup transsexuals: early and longterm surgical results. In: World Professional Association for Transgender Health Biennial Meeting, Chicago, 2007. Patientreported issues and practical outcomes of maletofemale intercourse reassignment surgery. Stress urinary incontinence after male to feminine gender reassignment surgical procedure: Successful use of a pubovaginal sling. To trigger coma, lesions of the diencephalon or brainstem must be bilateral, however could be quite focal in the occasion that they harm the ascending activating system near the midline in the midbrain or caudal diencephalon; cortical or subcortical damage must be each bilateral and diffuse. Both damaging and compressive lesions may trigger additional compression by producing brain edema. Most compressive lesions are treated surgically, whereas harmful lesions are usually handled medically. This article describes the pathophysiology and basic strategy to sufferers with structural lesions of the mind, first considering compressive and then damaging lesions. Chapter 2 described a variety of the bodily findings that distinguish structural from nonstructural causes of stupor and coma.
Dipyridamole 25 mg purchase mastercardThe following occasions occur: 1 Smooth muscles in the arteriolar and arterial partitions loosen up hypertension epidemiology dipyridamole 25 mg cheap without a prescription, leading to blood pressure 200 100 100 mg dipyridamole cheap with visa vascular dilation and increased blood circulate to the penis. This results in decreased venous outflow and will increase sinusoidal blood trapping and engorgement. Detumescence occurs when arterial inflow decreases as a result of easy muscle contraction. It has been described in three phases in the animal mannequin: 1 Initially, a transient enhance in intracorporeal pressure is noted as a outcome of easy muscle contraction against a closed venous system during erection. Central pathways Spinal pathways In the spinal wire, thoracolumbar sympathetic, sacral parasympathetic, and sacral pudendal motoneurons are concerned with erections. The thoracolumbar heart is mostly inhibitory to erections whereas parts of the sacral and pudendal promote erections. Supraspinal pathways Centers in the mind play a vital role in initiation, inhibition, and upkeep of erections by integrating and processing multiple sensory inputs. However, in addition to these centers, there are numerous different areas within the brain liable for regulation of erectile perform. These central structures are answerable for psychogenic, reflexogenic, and nocturnal erections. Sensory fibers will relay this information by way of ascending fibers to the brain, which processes this and prompts autonomic centers to produce an erection. Functional studies show elevated exercise within the pontine space, amygdalae, and anterior cingulate gyrus. Physiology of penile erection 2 this results in a sluggish decrease in corporeal strain as venous channels reopen as a end result of decreased mechanical compression. Additionally, contraction of the ischiocavernosus and bulbospongiosus muscular tissues promotes engorgement and will increase strain within the glans and spongiosum by compression of the spongiosum and penile veins through the rigid erection section. These additionally attenuate the dilatory effects of nitric oxide when released simultaneously, thus ren dering it much less effective. Thus, within the flaccid state, corporeal tissues are in a semicontracted state, which is attained via a mixture of intrinsic muscle exercise, adrenergic neurotransmission, and endotheliumderived components. Neurophysiology of erections Smooth muscle contraction and detumescence Sympathetic activity is conveyed by adrenergic recep tors. Specifically, postsynaptic 1a and 1d receptors and presynaptic 2 receptors convey sympathetic stimulation to induce contraction of easy muscular tissues. The sympathetic nerves induce detumescence and preserve penile flaccidity by rising sarcoplasmic free calcium (Ca2+) ranges, which promotes easy muscle contraction. Presynaptic 2adrenergic receptors increase extra cellular calcium entry via membrane ion channels, and 1 receptors release sequestered intracellular calcium in addition to selling entry of extracellular calcium. This leads to muscle contraction and upkeep of contractile tone, as mentioned under. Additionally, endothelin1, which is synthesized and present in sinusoidal endothelial tissues, acts as a vasoconstrictor. It additionally potentiates the constrictor response to catecholamines on the sinusoidal endo thelial tissue. These direct and oblique mechanisms recommend endothelin1 is concerned in detumescence. Specifically, serotonergic receptors could inhibit sexual function, sexual drive, and erections, whereas dopaminergic enter, by way of D1, D2, and D4 recep tors, and adrenergic receptors promotes sexual operate. For instance, apomorphine, which has D1 and D2 receptor activity, induces erectionabsent sexual stimu lation. Studies have demonstrated spontaneous contractile exercise in clean muscle, which can also be exercise induced. Ca2+ binds to calmodulin, a calciumbinding messenger pro tein, which triggers a cascade of events permitting myosin to crosslink to actin and contract the muscle. This is achieved via the motion of different vasoconstrictor brokers on their specific receptors, which activates a Gprotein coupled receptor (Gq). Activation of this results in a downstream cascade that will increase intracellular cyto solic calcium. To further improve intracellular calcium, constricting brokers additionally open calciumpermeable nonselective channels, permitting entry of extracellular Ca2+ as nicely. All of these processes improve sarcoplasmic Ca2+ permitting it to work together with calmodulin and trigger easy muscle contraction essential to maintain flaccidity and trigger detumescence. These activate specific protein kinases that phosphorylate downstream ion channels and pro teins. This leads to cell hyperpolarization by opening membrane potassium channels, sequestration of calcium to the endoplasmic reticulum, and inhibition of membrane calcium channels. These occasions result in decreased intracellular calcium, smooth muscle relaxa tion, and ultimately tumescence. This dephosphorylation adjustments the conformation of the myosin head so it not crosslinks with actin. It results in easy muscle relaxation and erection by phosphorylating downstream targets. Summary Thus, the advanced interplay between the central and peripheral nervous systems, penile anatomy, and neurotransmitters tightly regulates tumescence and detumescence. Erections depend upon the relief of cavernous and vascular easy muscle tissue from their ton ically contracted state. It is the inhibition of this enzyme that has been used as a therapeutic for erectile dysfunction. Advances in understanding of mammalian penile evolution, human penile anatomy and human erection physiology: scientific implications for physicians and surgeons. Brain processing of visual sexual stimuli in healthy males: a practical magnetic reso nance imaging study. A thorough understanding of the traditional mechanisms that mediate penile erection enables the provider to counsel and deal with male sufferers with sexual concerns. The tunica albuginea consists of multiple layers of collagen and elastic fibers, oriented in an internal circular and an outer longitudinal layer. This framework permits rigidity and axial energy during penile erection, and compliance and suppleness when the penis is flaccid. Distally, the corpus spongiosum forms a broad cap of erectile tissue called the glans penis, which covers the tips of corpora cavernosa. Penile anatomy the penis consists of three erectile our bodies: two corpora cavernosa and one corpus spongiosum. They are connected via an incomplete midline septum composed of a number of strands of connective tissue; the septum becomes more complete towards the distal aspect of the penis. A sheath of connective tissue referred to as the tunica Vascular anatomy the blood provide to the penis originates from the paired penile arteries, that are derived from the interior pudendal arteries and inside iliac arteries. The penile arteries travel alongside the medial border of the pubic rami after which proceed along the urethra bulb. The bulbourethral artery is the first branch of the penile artery; the dorsal artery of the penis is the continuation of the common penile artery. The dorsal artery courses deep to dorsal penile vein and lateral to the cavernous nerves. The dorsal artery offers off circumflex branches across the lateral floor of the Corporal bodies.
100 mg dipyridamole cheap overnight deliveryIn consequence heart attack 90 blockage buy dipyridamole 100 mg overnight delivery, m enstruation ceases and this inhibits urther progress o the lesions and perm its the body de enses to take up the contents o the lesions arrhythmia ablation is a treatment for quizlet 100 mg dipyridamole purchase visa. At laparoscopy the extent o the disease ought to be determ ined, as this can inf uence the treatm ent (Table 35. Danazol is given or 3�6 m onths, relying on the extent o the lesions and on the response. The sym ptom s are often relieved in 2�6 weeks in threequarters o wom en treated. Adverse e ects embody: � Am enorrhoea in 60% o wom en and oligom enorrhoea in the rem ainder � An improve in weight, o ten >3 kg � Oily pores and skin or acne in 20% o wom en � Deepening voice in 10% o wom en (irreversible) 290 Chapter 3 5 Endom etriosis and adenomyosis placebo a ter treatm ent is ceased. The results are: � In 30% o the wom en com plete regression o the illness may have occurred. Once horm onal treatm ent ceases, the m ean period or pain to recur is 5�6 m onths. It must be famous that the m ore in depth the disease the larger the chance o recurrence. Due to the facet e ects danazol is simply recom m ended i other treatm ents have been unsuccess ul. Adverse e ects embody: � Nearly all wom en experience hot f ushes, which m ay be extreme. Surg e ry Sm all lesions detected with laparoscopy can be handled by diathermy or laser ablation underneath laparoscopic vision. Larger lesions, notably these involving the ovaries, require m ore extensive surgical procedure. Spontaneous being pregnant rates within the 12 m onths ollowing surgical procedure seem above 50% and range according to severity. Gestrinone Gestrinone is a progestogen with m ixed agonist and antagonist e ects and has actions sim ilar to these o other androgen analogues, together with danazol, but with ewer side e ects. Side e ects o nausea, weight gain, oily hair, zits and m ood disturbances are com m on. Complementary treatments There is a paucity o good evidence on the e ectiveness o such treatm ents as acupuncture, hom eopathy, ref exology, traditional Chinese m edicine, natural treatm ents, vitam in B1 and m agnesium. The di erentiation between endom etriosis and the prem enstrual syndrom e needs to be mentioned because som e sym ptom s are sim ilar. The relationship between endom etriosis and in ertility needs to be mentioned and treatm ent methods outlined. The wom an should be m ade aware o the choices o horm onal treatm ent and surgical procedure (or a com bination o the two), and o their relative m erits in her case. The act that endom etriosis m ay recur ollowing either treatm ent needs to be delivered to her attention. However, the physician ought to o er quali ed optim ism concerning the outcom e, and may stress the im portance o adequate ollow-up. Note the thickened, heterogeneous anterior and posterior myometrium and the poorly demarcated myometrium�endometrium interface. Clinically, adenomyosis m ay be indistinguishable rom a leiomyom a, and both m ay coexist. Uterine artery em bolization is getting used increasingly as an alternative or wom en wishing to preserve their ertility. In the rem ainder the m ain sym ptom s are: � Progressively growing pain, often associated with m enstruation. In this case the pain will increase all through m enstruation, reaching its peak in direction of the latter phases. The m ost caudal portion, which is ready to becom e the vagina, becom es strong and fuses with an ingrowth of endoderm al cells from the cloaca. The error m ay be one of failure of the recanalization course of, or m ay be a failure of the two M�llerian ducts to fuse. Treatm ent is to m ake a cruciate incision in the hym en septum and perm it the inspissated uid to escape slowly. Benign tum ours occur m ost often in the uterus and m ost benign cysts occur in the ovaries. A subseptate uterus m ay lead to recurrent abortion, and could be handled by excising the septum by surgical procedure or laser. If the wom an has a bicornuate uterus and becom es pregnant, the fetus m ay current as a transverse lie in late being pregnant. A few wom en develop vulval varicosities, which m ay cause discom fort and are m ore m arked in pregnancy. A cystic swelling m ay happen within the anterior wall of the vagina, immediately below the urethra: it is a urethral diverticulum. If it becom es contaminated, the wom an com plains of dysuria and frequency of urination. The colum nar epithelium masking the polyp m ay undergo squam ous m etaplasia, or ulcerate. The m ain sym ptom s are interm ittent or postcoital bleed ing, although m any cervical polyps are sym ptom much less. The polyp may be rem oved by twisting the pedicle, and the tissue must be despatched for histopathology. Other tum ours that m ay be detected sometimes are genital pap illom ata and broids. Encapsulated easy muscle f bres interspersed with strands o connective tissue often creating within the myometrium. Dependent on an intact blood supply Unclear Increases rom 5�20% o girls during their reproductive years. Regress a ter menopause Examination and conf rmatory ultrasound Depend on measurement and position and are requently symptomless. A uterine broid is com posed of sm ooth m uscle bundles interspersed with strands of connective tissue, surrounded by a thin capsule (Box 36. The tum our m ay come up in any part of the M�llerian duct, but occurs m ost usually in the myom etrium, where several m ay develop sim ultaneously. They grow slowly and m ay only be detect able clinically within the fourth decade of life, when the incidence increases to about 20%. They m ay arise from norm al m uscle cells, from im m ature m uscle cells in the myo m etrium, or from em bryonal cells within the partitions of uterine blood vessels. Whatever their origin, the tum ours start as tiny m ultiple seedlings that are scattered via the myom etrium. At rst the tum our is intram ural, however because it grows it m ay develop in a number of instructions. After the m enopause, as oestrogen is now not secreted in any nice quantity, broids tend to atrophy. The bundles o spindle-shaped muscle cells run in several directions and tend to orm a whorl-like pattern.
100 mg dipyridamole purchase mastercardReduction of strain Cylinders contain gases at very high pressures (see earlier) that may range depending on the con tent or temperature of the cylinder hypertension readings 100 mg dipyridamole cheap free shipping. The gasoline from a cylinder passes through a decreasing valve to be certain that a relentless flow of fuel at 400 kPa is delivered to the flowmeters arrhythmia nclex dipyridamole 100 mg purchase free shipping. As piped gases are already deliv ered at four hundred kPa, no additional strain reduction is required. A particular, calibrated flowmeter is used for every gasoline and flow is managed by a needle valve. A rotating bobbin floats within the gasoline stream, its upper edge indicating the speed of gas circulate. On fashionable anaesthetic machines, flowmeters have been replaced with electronic management of gasoline move. The anaesthetist simply dials in the required move and gasoline composition and that is delivered into the anaesthetic breathing system. The flow of fuel is then displayed on a monitor display both numeri cally or as a digital illustration of a flowmeter. Historically, a selection of completely different respiratory systems were used but these days these have largely been changed by circle methods. The details of those systems are beyond the scope of this book but they all have a variety of widespread features, described later. As a number of sufferers in succession may breathe via the identical system, a lowresistance, disposable bacterial filter is positioned on the affected person finish of the system, and adjusted between every patient to scale back the risk of crossinfection. Alternatively, a disposable system can be used, which is changed between every patient. It additionally acts as a further safety system, being easily distended at low strain if obstruction occurs. During spontaneous air flow, resistance to opening is minimal so as to not impede expiration. Closing the valve and squeezing the reservoir bag permits the generation of optimistic strain inside the breathing system and therefore handbook ventilation of the affected person. Note the interlock positioned between the coloured dials to stop simultaneous supply of both vapours. This would lead to a fall within the concentration of anaesthetic delivered to the patient. To circumvent this problem, vaporizers incorporate a mechanism to compensate for the fall in temperature. This is usually a mechanical system that forestalls more than one vaporizer being turned on simultaneously. The resultant combination of gases and vapour is finally deliv ered to a typical outlet on the anaesthetic machine. From this level, specialised breathing techniques are used to transfer the gases and vapours to the affected person. The circle system Many traditional anaesthetic breathing systems used high flows of gases and vapour to forestall rebreathing of expired gases and hypercapnia. Most of the parts shown within the diagram are built-in; solely the inspiratory and expiratory tubing, the reservoir bag and soda lime container are apparent. Its composition is affected by a number of elements together with uptake of anaesthetic by the affected person and recent gas circulate. Anaesthetic equipment and monitoring 35 Patients can both breathe spontaneously or be ventilated when utilizing the circle system. Mechanical ventilation A broad number of anaesthetic ventilators is available, each of which capabilities in a slightly different way. The following is a top level view of the rules of mechanical ventilation; more details are available in the Further information section at the end of the chapter. During spontaneous air flow, adverse intratho racic stress is generated, inflicting gas to move into the lungs. A optimistic strain is utilized to the anaesthetic gases to overcome airway resistance and elastic recoil of the chest, inflicting gasoline flow into the lungs. In order to generate the optimistic strain, the ventilator requires a supply of power � usually gasoline pressure or electricity. In both spontaneous and mechanical air flow, expiration happens by passive recoil of the lungs and chest wall. Modes of ventilation Anaesthetists can choose the tidal quantity that they want the ventilator to ship to the affected person. The alternative is to set the maximum air way pressure generated by the ventilator. Whilst its use reduces the chance of barotrauma, it may lead to the supply of extreme tidal volumes, leading to volutrauma. This is used when the patient is respiration spontaneously but their very own res piratory effort leads to insufficient tidal volumes. In this case, the anaesthetist can set the ventilator to detect a spontaneous breath and then provide somewhat constructive pressure to assist improve the tidal volume. Some machines permit the vapour concentration to be set; on others, the focus from the vaporizer is about and adjusted to achieve the required endtidal concentration. All of the above are monitored and 36 Anaesthetic equipment and monitoring is utilized to the expiratory valve of the breathing system or ventilator to remove gases to the skin environment. The patient is protected in opposition to exces sive negative pressure being applied to the lungs by valves with very low opening pressures. Unfortunately, both nitrous oxide and, to a lesser extent, the inhalational anaesthetics are potent destroyers of ozone, thereby including to the greenhouse impact. All patients present process anaesthesia need intrave nous entry in order to administer fluids, blood and drugs. The exterior diameter is quoted by means of its gauge (G), and likewise in milli metres, and the utmost flow fee is often quoted on the packet. It consists of a plastic cannula mounted on a steel needle with the bevel protruding. Peripheral devices are available and are normally of enormous diameter for use when massive flow rates are needed. Some patients could require an arterial line for shut monitoring of their blood strain (see later). The first resembles a cannula over needle intravenous cannula except that the valved injection port is removed (to prevent mistaken intraarterial drug Minimizing theatre pollution Unless particular measures are taken, the atmosphere in the operating theatre would turn out to be polluted with anaesthetic gases. The respiratory techniques and mechanical ventilators described vent varying volumes of extra and expired gasoline into the atmos phere, the affected person expires anaesthetic gasoline during restoration and there are leaks from anaesthetic appara tus. Although no conclusive evidence exists to hyperlink prolonged publicity to low concentrations of inhala tional anaesthetics with any dangers, it will appear wise to minimize the degree of pollution inside the operating theatre setting. Scavenging techniques these gather the gas vented from respiratory techniques and ventilators and ship it via a pipeline system to the exterior environment. Once the needle is withdrawn from the cannula, the tip is protected to reduce the chance of a needlestick injury. This is compounded by the loss of physique temperature regulation and inabil ity to shiver when anaesthetized.
Generic dipyridamole 25 mg lineMisoprostol 800 �g is given intravaginally 5�7 days later pulse pressure range elderly order 25 mg dipyridamole overnight delivery, and following this 75% of wom en abort within 24 hours blood pressure youtube 100 mg dipyridamole purchase with visa. These regim ens induce an abortion in 90% of sufferers and m ay exchange dilatation of the cervix and uterine evacu ation using sponge forceps and a curette, which can be a bloody and extended process. Following the abortion, 10% of wom en require evacuation of the uterus for retained prod ucts of conception. Less than 1% of wom en develop infection, and the m ortality rate is lower than 1 per 100,000 abortions. After the twelfth gestational week the speed of com plications rises to 3�5% and the m ortality increases to 9�12 per one hundred,000. Most of the wom en adversely affected had been am bivalent about having the abortion, or felt pressured by dad and mom or associate into time period inating the preg nancy. This nding em phasizes that a wom an looking for an abortion ought to be counselled earlier than the process takes place, and may continue to receive assist (if she chooses) throughout and after the operation. Prem ature im plantation may occur if the passage of the fertilized ovum along the Fallopian tube is delayed due to tubal dam age following an infection. Most extra-uterine pregnancies happen within the Fallopian tubes (ectopic gestation) but, hardly ever, the fertilized ovum m ay im plant onto the ovarian floor or the uterine cervix. Extrem ely rarely, the fertilized ovum im vegetation onto the om entum (abdom inal pregnancy). One in ninety pregnancies is ectopic, and in the United Kingdom this results in the dying of 2�4 wom en annually. Whereas the rupture 113 Fundam entals of Obstetrics and Gynaecology In ampulla 55% In interstitial portion 2% Fallopian tube In isthmus 25% In ovary zero. The trophoblast burrows deeply and eventually erodes the serosal coat of the tube, the nal break being sudden or gradual. A few of these pregnancies advance to term and, in a very few, the fetus dies early and is transformed into a lithopaedion. The pain is decrease abdom inal in website, but not distinguishable from that of abortion. However, in ruptured ectopic gestation fainting normally happens, although this m ay solely be m om entary. Vaginal bleeding follows the ache, and m ay be m istaken for bleeding due to a delayed m enstrual interval or an abortion. The bleeding is a slightly brownish colour and continuous, and clots are not often present (Table 12. Two medical patterns happen and are due to the extent of the dam age to the tubal wall by the invading trophoblast. Further episodes of pain are doubtless and the blood loss per vaginam persists until acute collapse supervenes (indicating tubal rupture or incom plete tubal abortion) or the sym ptom s cease (indicating com plete abortion with or without a pelvic haem atocele). It is m ore ordinary for the acute rupture to supervene upon the subacute, however the m ild sym ptom s of the latter m ay have been thought to be norm al occurrences in pregnancy and ignored. As the tube ruptures the affected person is seized with a sudden acute decrease abdom inal ache, suf ciently severe to cause fainting. The related inner haem orrhage results in collapse, pallor, a weak, rapid pulse and a falling blood pressure. Usually the situation im proves after a brief tim e as the haem orrhage dim inishes or ceases, but abdom inal discom fort persists, and pain is felt in the epigastrium or is referred to the shoulder. A further episode of haem orrhage and collapse is likely, and continued bleeding may be suspected from rising pallor and a falling haem oglobin degree. On exam ination the affected person is in shock and the lower abdom en is tender, with som e fullness and m uscle 116 Chapter 1 2 Extra-uterine pregnancy/ectopic gestation guarding. Vaginal exam ination, which ought to solely be carried out in hospital, shows extrem e tenderness on m ovem ent of the cervix from aspect to aspect. If she is in shock, an intravenous line must be set up and transfer rapidly arranged. Once the ectopic gestation has been diagnosed, the treatm ent is often surgical or in selected instances m edical. The gynaecologist m ay: � Insert a laparoscope to examine the Fallopian tube and, if attainable, under laparoscopic imaginative and prescient incise along the superior border and suck the ectopic gestation out of the tube. The levels ought to double each forty eight hours, an increase <66% being suggestive of an ectopic gestation. On the other hand, if ultrasound exhibits an intra-uterine pregnancy, a concurrent ectopic pregnancy is extrem ely unlikely. Routine serum progesterone ranges might help to exclude an ectopic pregnancy (>79 nm ol/L) and identify a nonviable being pregnant (>15. If the wom an com plains of constant sym ptom s, a second-look laparoscopy m ay be necessary. The presence of contralateral tubal dam age from infection signi cantly reduces the possibilities of a profitable conception. In a subsequent pregnancy the chance of a second ectopic gestation is 10�20% com pared with a threat of 1% in different wom en. The bleeding occurs when the decrease uterine segm ent is increasing in length, and shearing forces between the trophoblast and the m aternal blood sinuses occur. The rst episode of bleeding happens after the thirty sixth gestational week in 60% of cases, between the thirty second and 36th weeks in 30%, and before the thirty second week in 10%. A additional ultrasound exam ination should be m ade at concerning the 32nd week, or earlier if vaginal bleeding occurs. Antepartum haem orrhage is de ned as signi cant bleeding from the start canal occurring after the twentieth week of pregnancy. The causes and proportions of cases of antepartum haem orrhage are proven in Table 13. The abdom en is palpated gently to determ ine the gestational age of the fetus, and its presentation and place. An ultrasound exam ination is m ade quickly after adm ission, to con rm the prognosis. Further m anagem ent depends on the severity of the bleeding and the gestational age of the fetus. In circumstances of extreme bleeding, pressing treatm ent to ship the child (and the placenta) is required, regardless of the a hundred and twenty Chapter 1 3 Antepartum haem orrhage gestational age of the fetus. If the bleeding is less severe, expectant treatm ent is suitable if the fetal gestational age is lower than 36 weeks. As the bleeding tends to recur, serum ought to be held within the blood financial institution in case an urgent transfusion is required and the most secure possibility for the wom an is to rem ain in hospital. An episode of extreme bleeding m ay lead to pressing supply, but in m ost cases the pregnancy can proceed until 38 to 39 weeks. All however the m ost m inor levels of placenta praevia will require delivery by caesarean part.
|